
Page 9 - Allegacy 2019 Benefit Guide Full Time
P. 9
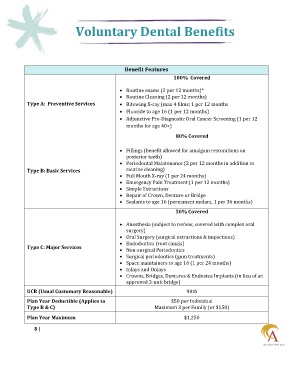
Voluntary Dental Benefits
Benefit Features
100% Covered
Routine exams (2 per 12 months)*
Routine Cleaning (2 per 12 months)
Type A: Preventive Services Bitewing X-ray (max 4 films; 1 per 12 months
Fluoride to age 16 (1 per 12 months)
Adjunctive Pre-Diagnostic Oral Cancer Screening (1 per 12
months for age 40+)
80% Covered
Fillings (benefit allowed for amalgam restorations on
posterior teeth)
Periodontal Maintenance (2 per 12 months in addition to
Type B: Basic Services routine cleaning)
Full Mouth X-ray (1 per 24 months)
Emergency Pain Treatment (1 per 12 months)
Simple Extractions
Repair of Crown, Denture or Bridge
Sealants to age 16 (permanent molars, 1 per 36 months)
50% Covered
Anesthesia (subject to review, covered with complex oral
surgery)
Oral Surgery (surgical extractions & impactions)
Endodontics (root canals)
Type C: Major Services
Non-surgical Periodontics
Surgical periodontics (gum treatments)
Space maintainers to age 16 (1 per 24 months)
Inlays and Onlays
Crowns, Bridges, Dentures & Endostea Implants (in lieu of an
approved 3-unit bridge)
UCR (Usual Customary Reasonable) 90th
Plan Year Deductible (Applies to $50 per Individual
Type B & C) Maximum 3 per Family (or $150)
Plan Year Maximum $1,250
8 |