
Page 15 - Jones and Frank Benefits Enrollments Guide
P. 15
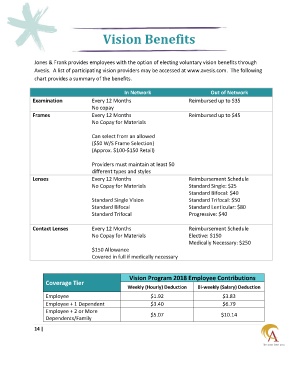
Vision Benefits
Jones & Frank provides employees with the option of electing voluntary vision benefits through
Avesis. A list of participating vision providers may be accessed at www.avesis.com. The following
chart provides a summary of the benefits.
In Network Out of Network
Examination Every 12 Months Reimbursed up to $35
No copay
Frames Every 12 Months Reimbursed up to $45
No Copay for Materials
Can select from an allowed
($50 W/S Frame Selection)
(Approx. $100-$150 Retail)
Providers must maintain at least 50
different types and styles
Lenses Every 12 Months Reimbursement Schedule
No Copay for Materials Standard Single: $25
Standard Bifocal: $40
Standard Single Vision Standard Trifocal: $50
Standard Bifocal Standard Lenticular: $80
Standard Trifocal Progressive: $40
Contact Lenses Every 12 Months Reimbursement Schedule
No Copay for Materials Elective: $150
Medically Necessary: $250
$150 Allowance
Covered in full if medically necessary
Vision Program 2018 Employee Contributions
Coverage Tier
Weekly (Hourly) Deduction Bi-weekly (Salary) Deduction
Employee $1.92 $3.83
Employee + 1 Dependent $3.40 $6.79
Employee + 2 or More
$5.07 $10.14
Dependents/Family
14 |