
Page 18 - ED draft
P. 18
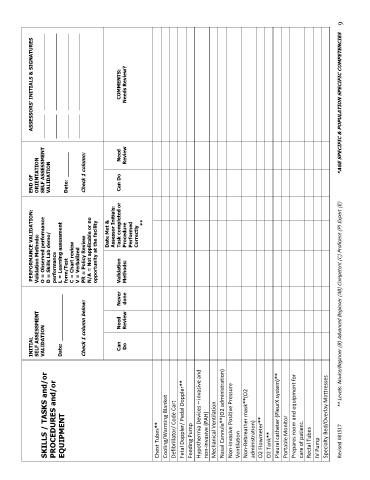
INITIAL PERFORMANCE VALIDATION: END OF ASSESSORS’ INITIALS & SIGNATURES
Validation Methods:
SELF ASSESSMENT
ORIENTATION
SKILLS / TASKS and/or VALIDATION O = Observed performance SELF ASSESSMENT _________ _____________________________
PROCEDURES and/or D = Skills Lab demo/ VALIDATION _________ _____________________________
performance
EQUIPMENT Date: _______________ L = Learning assessment
form/Test Date: ________ _________ _____________________________
C = Chart review
V = Verbalized _________ _____________________________
Check 1 column below: PR = Policy Review Check 1 column:
N/A = Not applicable or no
opportunity at the facility
Date Met &
Assessor Initials:
Can Need Never Validation Task completed or Can Do Need COMMENTS:
Do Review done Methods: Procedure Review Needs Review?
Performed
Correctly
**
Chest Tubes**
Cooling/Warming Blanket
Defibrillator/ Code Cart
Fetal Doppler/ Pedal Doppler**
Feeding Pump
Hypothermia Devices – invasive and
non-invasive (PAH)
Mechanical Ventilation
Nasal Cannula**(O2 administration)
Non-invasive Positive Pressure
Ventilation
Non-Rebreather mask**(O2
administration)
O2 Flowmeter**
O2 Tank**
Pleural catheter (PleurX system)**
Portable Monitor
Prepares room and equipment for
care of patient.
Rectal Tubes
IV Pump
Specialty Bed/Overlay Mattresses
Revised 081517 ** Levels: Novice/Beginner (B) Advanced Beginner (AB) Competent (C) Proficient (P) Expert (E) *AGE SPECIFIC & POPULATION SPECIFIC COMPETENCIES 9