
Page 19 - ED draft
P. 19
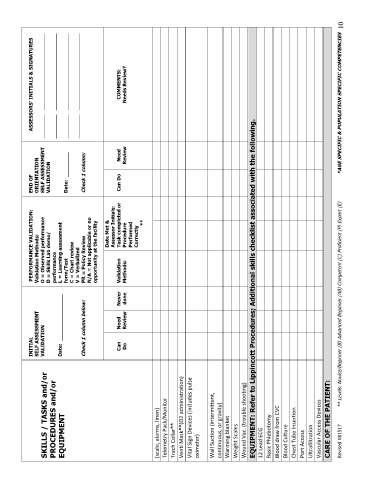
INITIAL PERFORMANCE VALIDATION: END OF ASSESSORS’ INITIALS & SIGNATURES
Validation Methods:
SELF ASSESSMENT
ORIENTATION
SKILLS / TASKS and/or VALIDATION O = Observed performance SELF ASSESSMENT _________ _____________________________
PROCEDURES and/or D = Skills Lab demo/ VALIDATION _________ _____________________________
performance
EQUIPMENT Date: _______________ L = Learning assessment
form/Test Date: ________ _________ _____________________________
C = Chart review
V = Verbalized _________ _____________________________
Check 1 column below: PR = Policy Review Check 1 column:
N/A = Not applicable or no
opportunity at the facility
Date Met &
Assessor Initials:
Can Need Never Validation Task completed or Can Do Need COMMENTS:
Do Review done Methods: Procedure Review Needs Review?
Performed
Correctly
**
(scale, alarms, linen)
Telemetry Pack/Monitor
Trach Collar**
Venti Mask**(O2 administration)
Vital Sign Devices (includes pulse
oximeter)
Wall Suction (intermittent,
continuous, or gravity)
Warming blanket
Weight Scales
Wound Vac. (trouble shooting)
EQUIPMENT: Refer to Lippincott Procedures; Additional skills checklist associated with the following.
12 Lead ECG
Basic Phlebotomy
Blood draw from CVC
Blood Culture
Chest Tube Insertion
Port Access
Ultrafiltration
Vascular Access Devices
CARE OF THE PATIENT:
Revised 081517 ** Levels: Novice/Beginner (B) Advanced Beginner (AB) Competent (C) Proficient (P) Expert (E) *AGE SPECIFIC & POPULATION SPECIFIC COMPETENCIES 10