
Page 21 - ED draft
P. 21
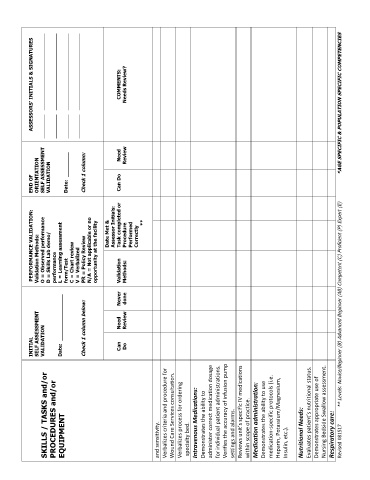
INITIAL PERFORMANCE VALIDATION: END OF ASSESSORS’ INITIALS & SIGNATURES
Validation Methods:
SELF ASSESSMENT
ORIENTATION
SKILLS / TASKS and/or VALIDATION O = Observed performance SELF ASSESSMENT _________ _____________________________
PROCEDURES and/or D = Skills Lab demo/ VALIDATION _________ _____________________________
performance
EQUIPMENT Date: _______________ L = Learning assessment
form/Test Date: ________ _________ _____________________________
C = Chart review
V = Verbalized _________ _____________________________
Check 1 column below: PR = Policy Review Check 1 column:
N/A = Not applicable or no
opportunity at the facility
Date Met &
Assessor Initials:
Can Need Never Validation Task completed or Can Do Need COMMENTS:
Do Review done Methods: Procedure Review Needs Review?
Performed
Correctly
**
and sensitivity.
Verbalizes criteria and procedure for
Wound Care Services consultation.
Verbalizes process for ordering
specialty bed.
Intravenous Medications:
Demonstrates the ability to
administer correct medication dosage
for individual patient administrations.
Verifies the accuracy of infusion pump
settings and alarms.
Reviews unit’s specific IV medications
within scope of practice.
Medication administration:
Demonstrates the ability to use
medication-specific protocols (i.e.
Heparin, Potassium/Magnesium,
Insulin, etc.).
Nutritional Needs:
Evaluates patient’s nutritional status.
Demonstrates appropriate use of
Nursing Bedside Swallow assessment.
Respiratory care:
Revised 081517 ** Levels: Novice/Beginner (B) Advanced Beginner (AB) Competent (C) Proficient (P) Expert (E) *AGE SPECIFIC & POPULATION SPECIFIC COMPETENCIES 12