
Page 20 - ED draft
P. 20
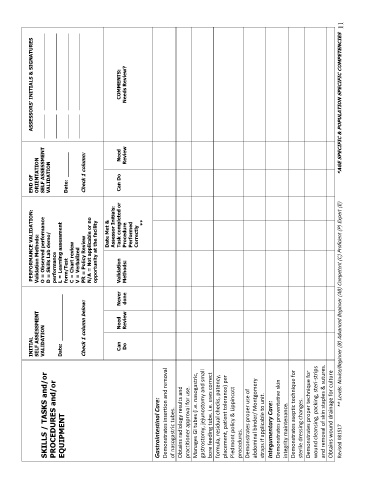
INITIAL PERFORMANCE VALIDATION: END OF ASSESSORS’ INITIALS & SIGNATURES
Validation Methods:
SELF ASSESSMENT
ORIENTATION
SKILLS / TASKS and/or VALIDATION O = Observed performance SELF ASSESSMENT _________ _____________________________
PROCEDURES and/or D = Skills Lab demo/ VALIDATION _________ _____________________________
performance
EQUIPMENT Date: _______________ L = Learning assessment
form/Test Date: ________ _________ _____________________________
C = Chart review
V = Verbalized _________ _____________________________
Check 1 column below: PR = Policy Review Check 1 column:
N/A = Not applicable or no
opportunity at the facility
Date Met &
Assessor Initials:
Can Need Never Validation Task completed or Can Do Need COMMENTS:
Do Review done Methods: Procedure Review Needs Review?
Performed
Correctly
**
Gastrointestinal Care:
Demonstrates insertion and removal
of nasogastric tubes.
Obtains radiology results and
practitioner approval for use.
Manages GI tubes (i.e. nasogastric,
gastrostomy, jejunostomy and small
bore feeding tube. i.e. uses correct
formula, residual checks, patency,
placement, patient tolerance) per
Piedmont policy & Lippincott
procedures.
Demonstrates proper use of
abdominal binder/ Montgomery
straps if applicable to unit.
Integumentary Care:
Demonstrates preventative skin
integrity maintenance.
Demonstrates aseptic technique for
sterile dressing changes.
Demonstrates proper technique for
wound cleansing, packing, steri-strips
and removal of skin staples & sutures.
Obtains wound drainage for culture
Revised 081517 ** Levels: Novice/Beginner (B) Advanced Beginner (AB) Competent (C) Proficient (P) Expert (E) *AGE SPECIFIC & POPULATION SPECIFIC COMPETENCIES 11