
Page 37 - MAPD_HMO_FLIP
P. 37
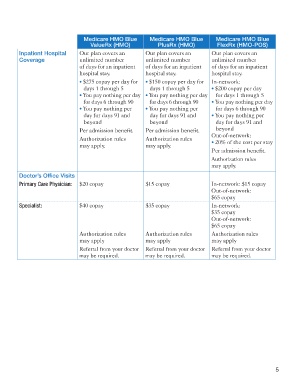
Medicare HMO Blue Medicare HMO Blue Medicare HMO Blue
ValueRx (HMO) PlusRx (HMO) FlexRx (HMO-POS)
Inpatient Hospital Our plan covers an Our plan covers an Our plan covers an
Coverage unlimited number unlimited number unlimited number
of days for an inpatient of days for an inpatient of days for an inpatient
hospital stay. hospital stay. hospital stay.
• $275 copay per day for • $150 copay per day for In-network:
days 1 through 5 days 1 through 5 • $200 copay per day
• You pay nothing per day • You pay nothing per day for days 1 through 5
for days 6 through 90 for days 6 through 90 • You pay nothing per day
• You pay nothing per • You pay nothing per for days 6 through 90
day for days 91 and day for days 91 and • You pay nothing per
beyond beyond day for days 91 and
Per admission benefit. Per admission benefit. beyond
Authorization rules Authorization rules Out-of-network:
• 20% of the cost per stay
may apply. may apply.
Per admission benefit.
Authorization rules
may apply.
Doctor’s Office Visits
Primary Care Physician: $20 copay $15 copay In-network: $15 copay
Out-of-network:
$65 copay
Specialist: $40 copay $35 copay In-network:
$35 copay
Out-of-network:
$65 copay
Authorization rules Authorization rules Authorization rules
may apply may apply may apply
Referral from your doctor Referral from your doctor Referral from your doctor
may be required. may be required. may be required.
5
5901 163138M-3_HMO Summary.indd 7 11/11/16 4:23 PM