
Page 39 - MAPD_HMO_FLIP
P. 39
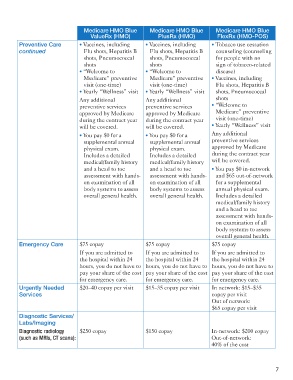
Medicare HMO Blue Medicare HMO Blue Medicare HMO Blue
ValueRx (HMO) PlusRx (HMO) FlexRx (HMO-POS)
Preventive Care • Vaccines, including • Vaccines, including • Tobacco use cessation
continued Flu shots, Hepatitis B Flu shots, Hepatitis B counseling (counseling
shots, Pneumococcal shots, Pneumococcal for people with no
shots shots sign of tobacco-related
• “Welcome to • “Welcome to disease)
Medicare” preventive Medicare” preventive • Vaccines, including
visit (one-time) visit (one-time) Flu shots, Hepatitis B
• Yearly “Wellness” visit • Yearly “Wellness” visit shots, Pneumococcal
Any additional Any additional shots
preventive services preventive services • “Welcome to
approved by Medicare approved by Medicare Medicare” preventive
during the contract year during the contract year visit (one-time)
will be covered. will be covered. • Yearly “Wellness” visit
• You pay $0 for a • You pay $0 for a Any additional
supplemental annual supplemental annual preventive services
physical exam. physical exam. approved by Medicare
Includes a detailed Includes a detailed during the contract year
medical/family history medical/family history will be covered.
and a head to toe and a head to toe • You pay $0 in-network
assessment with hands- assessment with hands- and $65 out-of-network
on examination of all on examination of all for a supplemental
body systems to assess body systems to assess annual physical exam.
overall general health. overall general health. Includes a detailed
medical/family history
and a head to toe
assessment with hands-
on examination of all
body systems to assess
overall general health.
Emergency Care $75 copay $75 copay $75 copay
If you are admitted to If you are admitted to If you are admitted to
the hospital within 24 the hospital within 24 the hospital within 24
hours, you do not have to hours, you do not have to hours, you do not have to
pay your share of the cost pay your share of the cost pay your share of the cost
for emergency care. for emergency care. for emergency care.
Urgently Needed $20–40 copay per visit $15–35 copay per visit In network: $15–$35
Services copay per visit
Out of network:
$65 copay per visit
Diagnostic Services/
Labs/Imaging
Diagnostic radiology $250 copay $150 copay In-network: $200 copay
(such as MRIs, CT scans): Out-of-network:
40% of the cost
7
5901 163138M-3_HMO Summary.indd 9 11/11/16 4:23 PM