
Page 1190 - Equine Clinical Medicine, Surgery and Reproduction, 2nd Edition
P. 1190
Eyes 1165
VetBooks.ir higher risk. Horses with white, grey or palomino 11.67
coat colours are predisposed. SCCs occur predomi-
nately in middle-aged to older horses. Tumours are
commonly located on the eyelid, nictitating mem-
brane, conjunctiva, cornea and/or limbus, in one or
both eyes. They are locally invasive and, rarely, will
metastasise to regional lymph nodes, salivary glands
and the lungs.
Aetiology/pathophysiology
The cause of ocular SCCs is unknown, but it is
likely to be multifactorial. Prolonged exposure to
ultraviolet (UV) radiation, increased altitude and
latitude, and non-pigmented or lightly pigmented
ocular and periocular structures appear to increase 11.68
susceptibility to SCC. Other pathogenic fac-
tors include exposure to mechanical irritants and
papillomavirus.
Although the pathophysiology is unknown,
lesions typically progress from non-cancerous
plaques to papillomas to carcinomas in situ prior to
transforming into SCC. These SCC tumours can
then invade locally and/or metastasise.
Clinical presentation
Clinical signs will depend on the anatomical loca-
tion and stage of development. Tumours may
appear as well-circumscribed, small, white, ele-
vated, hyperplastic plaques. Ocular SCCs may also 11.69
appear as raised, rough, irregular pinkish-white
warty or cauliflower-like structures with a broad
base of attachment. They can appear ulcerated
and necrotic, with lesions that may bleed easily
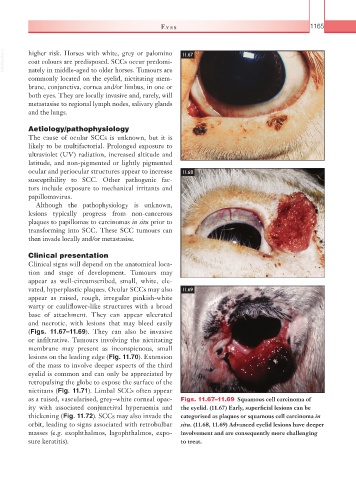
(Figs. 11.67–11.69). They can also be invasive
or infiltrative. Tumours involving the nictitating
membrane may present as inconspicuous, small
lesions on the leading edge (Fig. 11.70). Extension
of the mass to involve deeper aspects of the third
eyelid is common and can only be appreciated by
retropulsing the globe to expose the surface of the
nictitans (Fig. 11.71). Limbal SCCs often appear
as a raised, vascularised, grey–white corneal opac- Figs. 11.67–11.69 Squamous cell carcinoma of
ity with associated conjunctival hyperaemia and the eyelid. (11.67) Early, superficial lesions can be
thickening (Fig. 11.72). SCCs may also invade the categorised as plaques or squamous cell carcinoma in
orbit, leading to signs associated with retrobulbar situ. (11.68, 11.69) Advanced eyelid lesions have deeper
masses (e.g. exophthalmos, lagophthalmos, expo- involvement and are consequently more challenging
sure keratitis). to treat.