
Page 348 - Adams and Stashak's Lameness in Horses, 7th Edition
P. 348
314 Chapter 3
Lateral Medial Skin, subcutis
Level
VetBooks.ir P1A SDFT
DDFT
SSL
OSL
CSL
P1
Skin, subcutis
SDFT
P1B DDFT
SSL
OSL
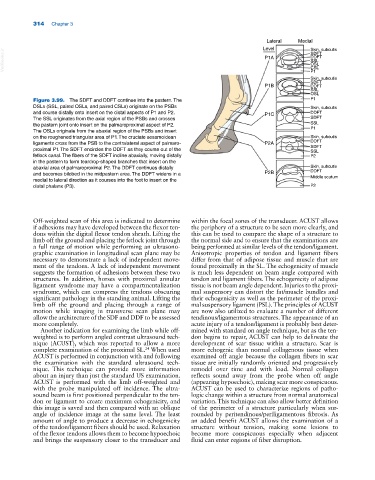
Figure 3.99. The SDFT and DDFT continue into the pastern. The P1
DSLs (SSL, paired OSLs, and paired CSLs) originate on the PSBs Skin, subcutis
and course distally onto insert on the distal aspects of P1 and P2. P1C DDFT
The SSL originates from the axial region of the PSBs and crosses SDFT
the pastern joint onto insert on the palmaroproximal aspect of P2. SSL
P1
The OSLs originate from the abaxial region of the PSBs and insert
on the roughened triangular area of P1. The cruciate sesamoidean Skin, subcutis
ligaments cross from the PSB to the contralateral aspect of palmaro P2A DDFT
SDFT
proximal P1. The SDFT encircles the DDFT as they course out of the SSL
fetlock canal. The fibers of the SDFT incline abaxially, moving distally P2
in the pastern to form teardrop‐shaped branches that insert on the
abaxial area of palmaroproximal P2. The DDFT continues distally Skin, subcutis
DDFT
and becomes bilobed in the midpastern area. The DDFT widens in a P2B Middle scutum
medial to lateral direction as it courses into the foot to insert on the
distal phalanx (P3). P2
Off‐weighted scan of this area is indicated to determine within the focal zones of the transducer. ACUST allows
if adhesions may have developed between the flexor ten the periphery of a structure to be seen more clearly, and
dons within the digital flexor tendon sheath. Lifting the this can be used to compare the shape of a structure to
limb off the ground and placing the fetlock joint through the normal side and to ensure that the examinations are
a full range of motion while performing an ultrasono being performed at similar levels of the tendon/ligament.
graphic examination in longitudinal scan plane may be Anisotropic properties of tendon and ligament fibers
necessary to demonstrate a lack of independent move differ from that of adipose tissue and muscle that are
ment of the tendons. A lack of independent movement found proximally in the SL. The echogenicity of muscle
suggests the formation of adhesions between these two is much less dependent on beam angle compared with
structures. In addition, horses with proximal annular tendon and ligament fibers. The echogenicity of adipose
ligament syndrome may have a compartmentalization tissue is not beam angle dependent. Injuries to the proxi
syndrome, which can compress the tendons obscuring mal suspensory can distort the fat/muscle bundles and
significant pathology in the standing animal. Lifting the their echogenicity as well as the perimeter of the proxi
limb off the ground and placing through a range of mal suspensory ligament (PSL). The principles of ACUST
motion while imaging in transverse scan plane may are now also utilized to evaluate a number of different
allow the architecture of the SDF and DDF to be assessed tendinous/ligamentous structures. The appearance of an
more completely. acute injury of a tendon/ligament is probably best deter
Another indication for examining the limb while off‐ mined with standard on angle technique, but as the ten
weighted is to perform angled contrast ultrasound tech don begins to repair, ACUST can help to delineate the
nique (ACUST), which was reported to allow a more development of scar tissue within a structure. Scar is
complete examination of the proximal SL. When used more echogenic than normal collagenous tissue when
24
ACUST is performed in conjunction with and following examined off angle because the collagen fibers in scar
the examination with the standard ultrasound tech tissue are initially randomly oriented and progressively
nique. This technique can provide more information remodel over time and with load. Normal collagen
about an injury than just the standard US examination. reflects sound away from the probe when off angle
ACUST is performed with the limb off‐weighted and (appearing hypoechoic), making scar more conspicuous.
with the probe manipulated off incidence. The ultra ACUST can be used to characterize regions of patho
sound beam is first positioned perpendicular to the ten logic change within a structure from normal anatomical
don or ligament to create maximum echogenicity, and variation. This technique can also allow better definition
this image is saved and then compared with an oblique of the perimeter of a structure particularly when sur
angle of incidence image at the same level. The least rounded by peritendinous/periligamentous fibrosis. As
amount of angle to produce a decrease in echogenicity an added benefit ACUST allows the examination of a
of the tendon/ligament fibers should be used. Relaxation structure without tension, making some lesions to
of the flexor tendons allows them to become hypoechoic become more conspicuous especially when adjacent
and brings the suspensory closer to the transducer and fluid can enter regions of fiber disruption.