
Page 1159 - Small Animal Internal Medicine, 6th Edition
P. 1159
CHAPTER 65 Disorders of the Spinal Cord 1131
of proprioception, delayed postural reactions, increased
BOX 65.1 extensor muscle tone, and normal to increased reflexes.
VetBooks.ir Common Spinal Cord Disorders When C6-T2 lesions are unilateral, ipsilateral forelimbs and
rear limbs will be affected. Horner syndrome may be seen if
the T1-T2 spinal cord segments or nerve roots are involved
Acute (Minutes to Hours)
External trauma (see Chapter 61), and the ipsilateral cutaneous trunci reflex
Hemorrhage/vascular infarction may be lost if the C8-T1 spinal cord segments or nerve roots
Type I intervertebral disk extrusion are damaged. Because the phrenic nerve originates at C5-C7,
Traumatic disk extrusion a severe lesion in this region could also cause diaphragmatic
Fibrocartilaginous embolism paralysis. When C6-T2 lesions affect only the central cord,
Atlantoaxial subluxation* the superficially located long tracts to the rear limbs are
Subacute Progressive (Days to Weeks) spared, so the forelimb LMN signs may be much more pro-
Infectious meningoencephalomyelitis nounced than the rear limb UMN signs.
Noninfectious inflammatory disease T3-L3 LESIONS
Granulomatous meningoencephalitis (GME), others
Aseptic meningitis (usually painful, normal neurologic Spinal cord lesions between segments T3 and L3 cause UMN
exam) paresis and ataxia affecting the rear limbs (see Table 65.1),
Diskospondylitis (usually painful, normal neurologic exam) but forelimbs are normal. Examination of the rear limbs
Type I intervertebral disk extrusion* reveals a long uncoordinated stride, loss of proprioception,
Rapidly growing tumors (lymphoma, metastatic neoplasia) delayed postural reactions, increased extensor muscle tone,
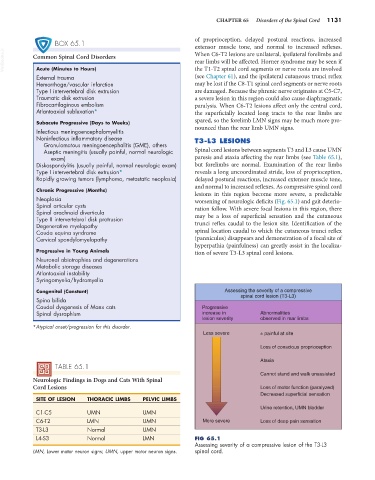
and normal to increased reflexes. As compressive spinal cord
Chronic Progressive (Months) lesions in this region become more severe, a predictable
Neoplasia worsening of neurologic deficits (Fig. 65.1) and gait deterio-
Spinal articular cysts ration follow. With severe focal lesions in this region, there
Spinal arachnoid diverticula
Type II intervertebral disk protrusion may be a loss of superficial sensation and the cutaneous
Degenerative myelopathy trunci reflex caudal to the lesion site. Identification of the
Cauda equina syndrome spinal location caudal to which the cutaneous trunci reflex
Cervical spondylomyelopathy (panniculus) disappears and demonstration of a focal site of
hyperpathia (painfulness) can greatly assist in the localiza-
Progressive in Young Animals tion of severe T3-L3 spinal cord lesions.
Neuronal abiotrophies and degenerations
Metabolic storage diseases
Atlantoaxial instability
Syringomyelia/hydromyelia
Congenital (Constant) Assessing the severity of a compressive
spinal cord lesion (T3-L3)
Spina bifida
Caudal dysgenesis of Manx cats Progressive
Spinal dysraphism increase in Abnormalities
lesion severity observed in rear limbs
*Atypical onset/progression for this disorder.
Less severe ± painful at site
Loss of conscious proprioception
Ataxia
TABLE 65.1
Cannot stand and walk unassisted
Neurologic Findings in Dogs and Cats With Spinal
Cord Lesions Loss of motor function (paralyzed)
Decreased superficial sensation
SITE OF LESION THORACIC LIMBS PELVIC LIMBS
Urine retention, UMN bladder
C1-C5 UMN UMN
C6-T2 LMN UMN More severe Loss of deep pain sensation
T3-L3 Normal UMN
L4-S3 Normal LMN FIG 65.1
Assessing severity of a compressive lesion of the T3-L3
LMN, Lower motor neuron signs; UMN, upper motor neuron signs. spinal cord.