
Page 353 - Canine Lameness
P. 353
19.4 Cranial Cruciate igament Disease 325
(A) (C) (E) (G)
(B) (D) (F) (H)
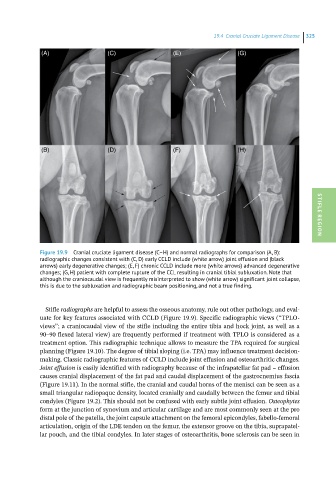
Figure 19.9 Cranial cruciate ligament disease (C–H) and normal radiographs for comparison (A, B): STIFLE REGION
radiographic changes consistent with (C, D) early CCLD include (white arrow) joint effusion and (black
arrows) early degenerative changes; (E, F) chronic CCLD include more (white arrows) advanced degenerative
changes; (G, H) patient with complete rupture of the CCL resulting in cranial tibial subluxation. Note that
although the craniocaudal view is frequently misinterpreted to show (white arrow) significant joint collapse,
this is due to the subluxation and radiographic beam positioning, and not a true finding.
Stifle radiographs are helpful to assess the osseous anatomy, rule out other pathology, and eval-
uate for key features associated with CCLD (Figure 19.9). Specific radiographic views (“TPLO-
views”; a craniocaudal view of the stifle including the entire tibia and hock joint, as well as a
90–90 flexed lateral view) are frequently performed if treatment with TPLO is considered as a
treatment option. This radiographic technique allows to measure the TPA required for surgical
planning (Figure 19.10). The degree of tibial sloping (i.e. TPA) may influence treatment decision-
making. Classic radiographic features of CCLD include joint effusion and osteoarthritic changes.
Joint effusion is easily identified with radiography because of the infrapatellar fat pad – effusion
causes cranial displacement of the fat pad and caudal displacement of the gastrocnemius fascia
(Figure 19.11). In the normal stifle, the cranial and caudal horns of the menisci can be seen as a
small triangular radiopaque density, located cranially and caudally between the femur and tibial
condyles (Figure 19.2). This should not be confused with early subtle joint effusion. Osteophytes
form at the junction of synovium and articular cartilage and are most commonly seen at the pro
distal pole of the patella, the joint capsule attachment on the femoral epicondyles, fabello-femoral
articulation, origin of the LDE tendon on the femur, the extensor groove on the tibia, suprapatel-
lar pouch, and the tibial condyles. In later stages of osteoarthritis, bone sclerosis can be seen in