
Page 24 - Confie Benefits Guide 01-18_FINAL_r2_dp wording
P. 24
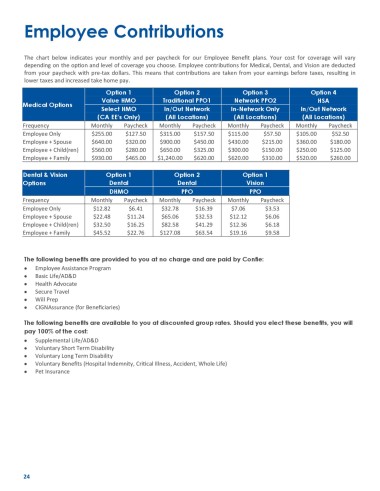
Employee Contributions
The chart below indicates your monthly and per paycheck for our Employee Benefit plans. Your cost for coverage will vary
depending on the option and level of coverage you choose. Employee contributions for Medical, Dental, and Vision are deducted
from your paycheck with pre-tax dollars. This means that contributions are taken from your earnings before taxes, resulting in
lower taxes and increased take home pay.
Option 1 Option 2 Option 3 Option 4
Value HMO Traditional PPO1 Network PPO2 HSA
Medical Options
Select HMO In/Out Network In-Network Only In/Out Network
(CA EE’s Only) (All Locations) (All Locations) (All Locations)
Frequency Monthly Paycheck Monthly Paycheck Monthly Paycheck Monthly Paycheck
Employee Only $255.00 $127.50 $315.00 $157.50 $115.00 $57.50 $105.00 $52.50
Employee + Spouse $640.00 $320.00 $900.00 $450.00 $430.00 $215.00 $360.00 $180.00
Employee + Child(ren) $560.00 $280.00 $650.00 $325.00 $300.00 $150.00 $250.00 $125.00
Employee + Family $930.00 $465.00 $1,240.00 $620.00 $620.00 $310.00 $520.00 $260.00
Dental & Vision Option 1 Option 2 Option 1
Options Dental Dental Vision
DHMO PPO PPO
Frequency Monthly Paycheck Monthly Paycheck Monthly Paycheck
Employee Only $12.82 $6.41 $32.78 $16.39 $7.06 $3.53
Employee + Spouse $22.48 $11.24 $65.06 $32.53 $12.12 $6.06
Employee + Child(ren) $32.50 $16.25 $82.58 $41.29 $12.36 $6.18
Employee + Family $45.52 $22.76 $127.08 $63.54 $19.16 $9.58
The following benefits are provided to you at no charge and are paid by Confie:
• Employee Assistance Program
• Basic Life/AD&D
• Health Advocate
• Secure Travel
• Will Prep
• CIGNAssurance (for Beneficiaries)
The following benefits are available to you at discounted group rates. Should you elect these benefits, you will
pay 100% of the cost:
• Supplemental Life/AD&D
• Voluntary Short Term Disability
• Voluntary Long Term Disability
• Voluntary Benefits (Hospital Indemnity, Critical Illness, Accident, Whole Life)
• Pet Insurance
24