
Page 10 - The Raymond Group Supplemental Benefit Guide
P. 10
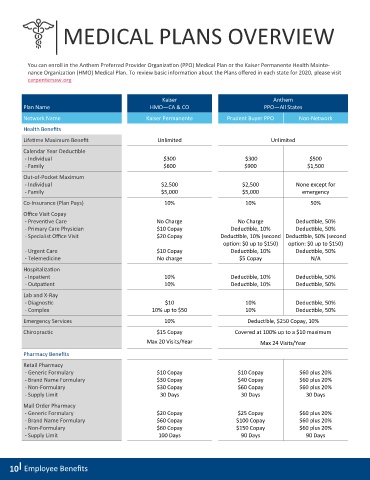
MEDICAL PLANS OVERVIEW
You can enroll in the Anthem Preferred Provider Organization (PPO) Medical Plan or the Kaiser Permanente Health Mainte-
nance Organization (HMO) Medical Plan. To review basic information about the Plans offered in each state for 2020, please visit
carpenterssw.org
Kaiser Anthem
Plan Name HMO—CA & CO PPO—All States
Network Name Kaiser Permanente Prudent Buyer PPO Non-Network
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited
Calendar Year Deductible
- Individual $300 $300 $500
- Family $600 $900 $1,500
Out-of-Pocket Maximum
- Individual $2,500 $2,500 None except for
- Family $5,000 $5,000 emergency
Co-Insurance (Plan Pays) 10% 10% 50%
Office Visit Copay
- Preventive Care No Charge No Charge Deductible, 50%
- Primary Care Physician $10 Copay Deductible, 10% Deductible, 50%
- Specialist Office Visit $20 Copay Deductible, 10% (second Deductible, 50% (second
option: $0 up to $150) option: $0 up to $150)
- Urgent Care $10 Copay Deductible, 10% Deductible, 50%
- Telemedicine No charge $5 Copay N/A
Hospitalization
- Inpatient 10% Deductible, 10% Deductible, 50%
- Outpatient 10% Deductible, 10% Deductible, 50%
Lab and X-Ray
- Diagnostic $10 10% Deductible, 50%
- Complex 10% up to $50 10% Deductible, 50%
Emergency Services 10% Deductible, $250 Copay, 10%
Chiropractic $15 Copay Covered at 100% up to a $10 maximum
Max 20 Visits/Year Max 24 Visits/Year
Pharmacy Benefits
Retail Pharmacy
- Generic Formulary $10 Copay $10 Copay $60 plus 20%
- Brand Name Formulary $30 Copay $40 Copay $60 plus 20%
- Non-Formulary $30 Copay $60 Copay $60 plus 20%
- Supply Limit 30 Days 30 Days 30 Days
Mail Order Pharmacy
- Generic Formulary $20 Copay $25 Copay $60 plus 20%
- Brand Name Formulary $60 Copay $100 Copay $60 plus 20%
- Non-Formulary $60 Copay $150 Copay $60 plus 20%
- Supply Limit 100 Days 90 Days 90 Days
10 Employee Benefits