
Page 6 - CW Driver Benefit Guide 2019 MAIN
P. 6
BENEFITS ENROLLMENT GUIDE
MEDICAL OPTIONS
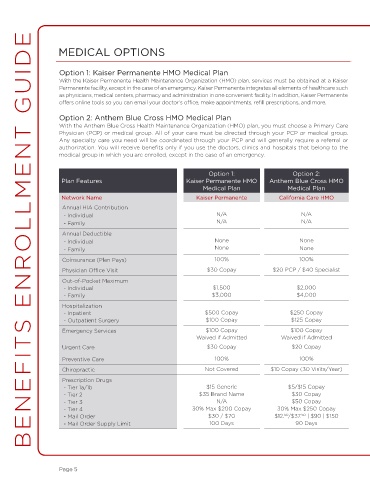
Option 1: Kaiser Permanente HMO Medical Plan
With the Kaiser Permanente Health Maintenance Organization (HMO) plan, services must be obtained at a Kaiser
Permanente facility, except in the case of an emergency. Kaiser Permanente integrates all elements of healthcare such
as physicians, medical centers, pharmacy and administration in one convenient facility. In addition, Kaiser Permanente
offers online tools so you can email your doctor’s office, make appointments, refill prescriptions, and more.
Option 2: Anthem Blue Cross HMO Medical Plan
With the Anthem Blue Cross Health Maintenance Organization (HMO) plan, you must choose a Primary Care
Physician (PCP) or medical group. All of your care must be directed through your PCP or medical group.
Any specialty care you need will be coordinated through your PCP and will generally require a referral or
authorization. You will receive benefits only if you use the doctors, clinics and hospitals that belong to the
medical group in which you are enrolled, except in the case of an emergency.
Option 1: Option 2:
Plan Features Kaiser Permanente HMO Anthem Blue Cross HMO
Medical Plan Medical Plan
Network Name Kaiser Permanente California Care HMO
Annual HIA Contribution
- Individual N/A N/A
- Family N/A N/A
Annual Deductible
- Individual None None
- Family None None
Coinsurance (Plan Pays) 100% 100%
Physician Office Visit $30 Copay $20 PCP / $40 Specialist
Out-of-Pocket Maximum
- Individual $1,500 $2,000
- Family $3,000 $4,000
Hospitalization
- Inpatient $500 Copay $250 Copay
- Outpatient Surgery $100 Copay $125 Copay
Emergency Services $100 Copay $100 Copay
Waived if Admitted Waived if Admitted
Urgent Care $30 Copay $20 Copay
Preventive Care 100% 100%
Chiropractic Not Covered $10 Copay (30 Visits/Year)
Prescription Drugs
- Tier 1a/1b $15 Generic $5/$15 Copay
- Tier 2 $35 Brand Name $30 Copay
- Tier 3 N/A $50 Copay
- Tier 4 30% Max $200 Copay 30% Max $250 Copay
50
- Mail Order $30 / $70 $12. /$37. | $90 | $150
50
- Mail Order Supply Limit 100 Days 90 Days
Page 5