
Page 14 - Palomar EE Guide 01-19 FINAL
P. 14
Health & Wellness
Vision Care Plan Name Vision
In-Network Non-Network
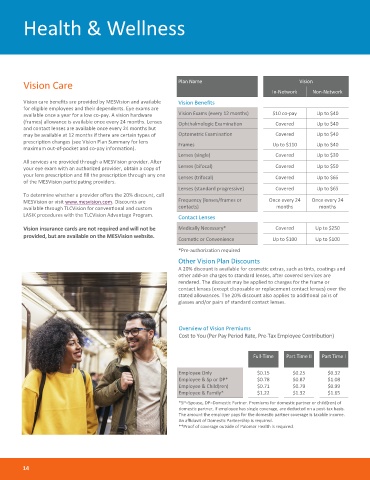
Vision care benefits are provided by MESVision and available Vision Benefits
for eligible employees and their dependents. Eye exams are
available once a year for a low co-pay. A vision hardware Vision Exams (every 12 months) $10 co-pay Up to $40
(frames) allowance is available once every 24 months. Lenses Ophthalmologic Examination Covered Up to $40
and contact lenses are available once every 24 months but
may be available at 12 months if there are certain types of Optometric Examination Covered Up to $40
prescription changes (see Vision Plan Summary for lens Frames Up to $110 Up to $40
maximum out-of-pocket and co-pay information).
Lenses (single) Covered Up to $30
All services are provided through a MESVision provider. After
your eye exam with an authorized provider, obtain a copy of Lenses (bifocal) Covered Up to $50
your lens prescription and fill the prescription through any one Lenses (trifocal) Covered Up to $65
of the MESVision participating providers.
Lenses (standard progressive) Covered Up to $65
To determine whether a provider offers the 20% discount, call
MESVision or visit www.mesvision.com. Discounts are Frequency (lenses/frames or Once every 24 Once every 24
available through TLCVision for conventional and custom contacts) months months
LASIK procedures with the TLCVision Advantage Program. Contact Lenses
Vision insurance cards are not required and will not be Medically Necessary* Covered Up to $250
provided, but are available on the MESVision website.
Cosmetic or Convenience Up to $100 Up to $100
*Pre-authorization required
Other Vision Plan Discounts
A 20% discount is available for cosmetic extras, such as tints, coatings and
other add-on charges to standard lenses, after covered services are
rendered. The discount may be applied to charges for the frame or
contact lenses (except disposable or replacement contact lenses) over the
stated allowances. The 20% discount also applies to additional pairs of
glasses and/or pairs of standard contact lenses.
Overview of Vision Premiums
Cost to You (Per Pay Period Rate, Pre-Tax Employee Contribution)
Full-Time Part Time II Part Time I
Employee Only $0.15 $0.25 $0.32
Employee & Sp or DP* $0.78 $0.87 $1.08
Employee & Child(ren) $0.71 $0.79 $0.99
Employee & Family* $1.22 $1.32 $1.65
*SP=Spouse, DP=Domestic Partner. Premiums for domestic partner or child(ren) of
domestic partner, if employee has single coverage, are deducted on a post-tax basis.
The amount the employer pays for the domestic partner coverage is taxable income.
An affidavit of Domestic Partnership is required.
**Proof of coverage outside of Palomar Health is required.
14