
Page 29 - Lyon Benefits Guide 01-18 National - FINAL
P. 29
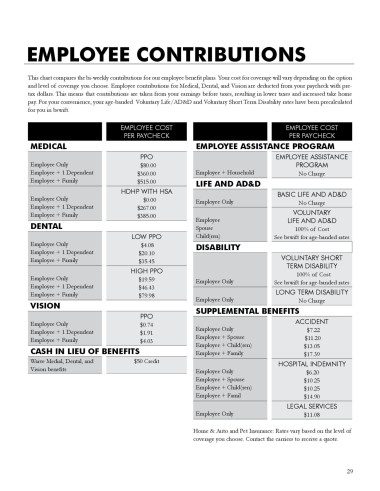
EMPLOYEE CONTRIBUTIONS
This chart compares the bi-weekly contributions for our employee benefit plans. Your cost for coverage will vary depending on the option
and level of coverage you choose. Employee contributions for Medical, Dental, and Vision are deducted from your paycheck with pre-
tax dollars. This means that contributions are taken from your earnings before taxes, resulting in lower taxes and increased take home
pay. For your convenience, your age-banded Voluntary Life/AD&D and Voluntary Short Term Disability rates have been precalculated
for you in bswift.
EMPLOYEE COST EMPLOYEE COST
PER PAYCHECK PER PAYCHECK
MEDICAL EMPLOYEE ASSISTANCE PROGRAM
PPO EMPLOYEE ASSISTANCE
Employee Only $80.00 PROGRAM
Employee + 1 Dependent $360.00 Employee + Household No Charge
Employee + Family $515.00 LIFE AND AD&D
HDHP WITH HSA BASIC LIFE AND AD&D
Employee Only $0.00 Employee Only No Charge
Employee + 1 Dependent $267.00
Employee + Family $385.00 Employee VOLUNTARY
DENTAL Spouse LIFE AND AD&D
100% of Cost
LOW PPO Child(ren) See bswift for age-banded rates
Employee Only $4.08 DISABILITY
Employee + 1 Dependent $20.10
Employee + Family $35.45 VOLUNTARY SHORT
HIGH PPO TERM DISABILITY
100% of Cost
Employee Only $19.59 Employee Only
Employee + 1 Dependent $46.43 See bswift for age-banded rates
Employee + Family $79.98 Employee Only LONG TERM DISABILITY
VISION SUPPLEMENTAL BENEFITS No Charge
PPO
Employee Only $0.74 ACCIDENT
Employee + 1 Dependent $1.91 Employee Only $7.22
Employee + Family $4.03 Employee + Spouse $11.20
Employee + Child(ren)
CASH IN LIEU OF BENEFITS Employee + Family $13.05
$17.39
Waive Medial, Dental, and $50 Credit HOSPITAL INDEMNITY
Vision benefits Employee Only $6.20
Employee + Spouse $10.25
Employee + Child(ren) $10.25
Employee + Famil $14.90
LEGAL SERVICES
Employee Only $11.08
Home & Auto and Pet Insurance: Rates vary based on the level of
coverage you choose. Contact the carriers to receive a quote.
29