
Page 1129 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 1129
CHAPTER 62 Drugs Used in the Treatment of Gastrointestinal Diseases 1115
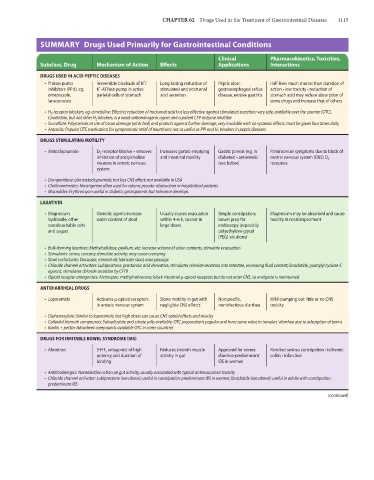
SUMMARY Drugs Used Primarily for Gastrointestinal Conditions
Clinical Pharmacokinetics, Toxicities,
Subclass, Drug Mechanism of Action Effects Applications Interactions
DRUGS USED IN ACID-PEPTIC DISEASES
+
• Proton-pump Irreversible blockade of H / Long-lasting reduction of Peptic ulcer, Half-lives much shorter than duration of
+
inhibitors (PPIs), eg, K -ATPase pump in active stimulated and nocturnal gastroesophageal reflux action • low toxicity • reduction of
omeprazole, parietal cells of stomach acid secretion disease, erosive gastritis stomach acid may reduce absorption of
lansoprazole some drugs and increase that of others
• H 2 -receptor blockers, eg, cimetidine: Effective reduction of nocturnal acid but less effective against stimulated secretion; very safe, available over the counter (OTC).
Cimetidine, but not other H 2 blockers, is a weak antiandrogenic agent and a potent CYP enzyme inhibitor
• Sucralfate: Polymerizes at site of tissue damage (ulcer bed) and protects against further damage; very insoluble with no systemic effects; must be given four times daily
• Antacids: Popular OTC medication for symptomatic relief of heartburn; not as useful as PPI and H 2 blockers in peptic diseases
DRUGS STIMULATING MOTILITY
• Metoclopramide D 2 -receptor blocker • removes Increases gastric emptying Gastric paresis (eg, in Parkinsonian symptoms due to block of
inhibition of acetylcholine and intestinal motility diabetes) • antiemetic central nervous system (CNS) D 2
neurons in enteric nervous (see below) receptors
system
• Domperidone: Like metoclopramide, but less CNS effect; not available in USA
• Cholinomimetics: Neostigmine often used for colonic pseudo-obstruction in hospitalized patients
• Macrolides: Erythromycin useful in diabetic gastroparesis but tolerance develops
LAXATIVES
• Magnesium Osmotic agents increase Usually causes evacuation Simple constipation; Magnesium may be absorbed and cause
hydroxide, other water content of stool within 4–6 h, sooner in bowel prep for toxicity in renal impairment
nonabsorbable salts large doses endoscopy (especially
and sugars polyethylene glycol
[PEG] solutions)
• Bulk-forming laxatives: Methylcellulose, psyllium, etc: increase volume of colon contents, stimulate evacuation
• Stimulants: senna, cascara; stimulate activity; may cause cramping
• Stool surfactants: Docusate, mineral oil; lubricate stool, ease passage
• Chloride channel activators: Lubiprostone, prostanoic acid derivative, stimulates chloride secretion into intestine, increasing fluid content; linaclotide, guanylyl cyclase-C
agonist, stimulates chloride secretion by CFTR
• Opioid receptor antagonists: Alvimopan, methylnaltrexone; block intestinal μ-opioid receptors but do not enter CNS, so analgesia is maintained
ANTIDIARRHEAL DRUGS
• Loperamide Activates μ-opioid receptors Slows motility in gut with Nonspecific, Mild cramping but little or no CNS
in enteric nervous system negligible CNS effects noninfectious diarrhea toxicity
• Diphenoxylate: Similar to loperamide, but high doses can cause CNS opioid effects and toxicity
• Colloidal bismuth compounds: Subsalicylate and citrate salts available. OTC preparations popular and have some value in travelers’ diarrhea due to adsorption of toxins
• Kaolin + pectin: Adsorbent compounds available OTC in some countries
DRUGS FOR IRRITABLE BOWEL SYNDROME (IBS)
• Alosetron 5-HT 3 antagonist of high Reduces smooth muscle Approved for severe Rare but serious constipation • ischemic
potency and duration of activity in gut diarrhea-predominant colitis • infarction
binding IBS in women
• Anticholinergics: Nonselective action on gut activity, usually associated with typical antimuscarinic toxicity
• Chloride channel activator: Lubiprostone (see above); useful in constipation-predominant IBS in women; linaclotide (see above): useful in adults with constipation-
predominant IBS
(continued)