
Page 15 - Cover Letter and evaluation for Michael Hartzmark
P. 15
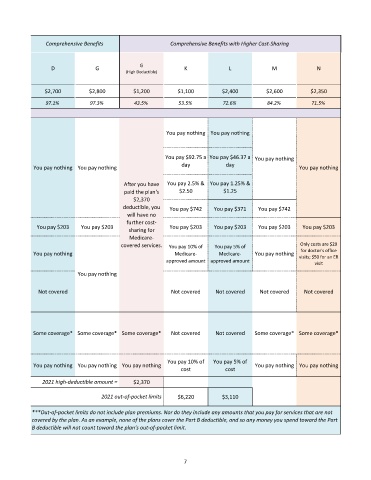
Comprehensive Benefits Comprehensive Benefits with Higher Cost-Sharing
D G G K L M N
(High Deductible)
$2,700 $2,800 $1,200 $1,100 $2,400 $2,600 $2,350
97.1% 97.3% 43.5% 53.5% 72.6% 84.2% 71.5%
You pay nothing You pay nothing
You pay $92.75 a You pay $46.37 a You pay nothing
You pay nothing You pay nothing day day You pay nothing
After you have You pay 2.5% & You pay 1.25% &
paid the plan's $2.50 $1.25
$2,370
deductible, you You pay $742 You pay $371 You pay $742
will have no
further cost-
You pay $203 You pay $203 sharing for You pay $203 You pay $203 You pay $203 You pay $203
Medicare-
covered services. You pay 10% of You pay 5% of Only costs are $20
for doctor's office
You pay nothing Medicare- Medicare- You pay nothing visits; $50 for an ER
approved amount approved amount visit
You pay nothing
Not covered Not covered Not covered Not covered Not covered
Some coverage* Some coverage* Some coverage* Not covered Not covered Some coverage* Some coverage*
You pay 10% of You pay 5% of
You pay nothing You pay nothing You pay nothing You pay nothing You pay nothing
cost cost
2021 high-deductible amount = $2,370
2021 out-of-pocket limits $6,220 $3,110
***Out-of-pocket limits do not include plan premiums. Nor do they include any amounts that you pay for services that are not
covered by the plan. As an example, none of the plans cover the Part B deductible, and so any money you spend toward the Part
B deductible will not count toward the plan's out-of-pocket limit.
7