Page 4 - Summit BHC 2022 Benefits Guide Summit Corporate
P. 4
Medical
BlueCross BlueShield of Tennessee
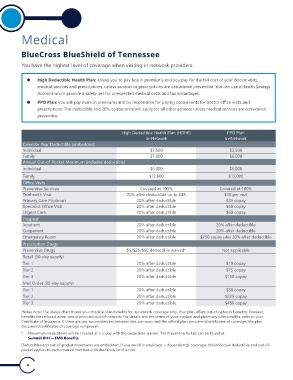
You have the highest level of coverage when visiting in-network providers.
z High Deductible Health Plan: allows you to pay less in premiums and you pay for the full cost of your doctor visits,
medical services and prescriptions, unless services or prescriptions are considered preventive. You can use a Health Savings
Account which provide a safety net for unexpected medical costs and tax advantages.
z PPO Plan: you will pay more in premiums and be responsible for paying copayments for doctor oice visits and
prescriptions. The deductible and 20% coinsurance will apply for all other services unless medical services are considered
preventive.
High Deductible Health Plan (HDHP) PPO Plan
In-Network In-Network
Calendar Year Deductible (embedded)
Individual $3,500 $2,500
Family $7,000 $6,000
Annual Out-of-Pocket Maximum (includes deductible)
Individual $6,000 $6,000
Family $12,000 $12,000
Oice Visits
Preventive Services Covered at 100% Covered at 100%
Telehealth Visit 20% after deductible up to $45 $10 per visit
Primary Care Physician 20% after deductible $35 copay
Specialist Oice Visit 20% after deductible $60 copay
Urgent Care 20% after deductible $60 copay
Hospital
Inpatient 20% after deductible 20% after deductible
Outpatient 20% after deductible 20% after deductible
Emergency Room 20% after deductible $250 copay plus 20% after deductible
Prescription Drugs
Preventive Drugs $5/$25/$50 deductible waived* Not applicable
Retail (30-day supply)
Tier 1 20% after deductible $10 copay
Tier 2 20% after deductible $75 copay
Tier 3 20% after deductible $150 copay
Mail Order (90-day supply)
Tier 1 20% after deductible $30 copay
Tier 2 20% after deductible $225 copay
Tier 3 20% after deductible $450 copay
Please note: The above chart shows your medical plan beneits for in-network coverage only. Your plan ofers out-of-network beneits; however,
beneits are reduced when care is provided out-of-network. For details and the terms of your medical and pharmacy plan beneits, refer to your
Certiicate of Insurance. If there are any inconsistencies between this summary and the oicial plan document/certiicates of coverage, the plan
document/certiicates of coverage will prevail.
* Preventive medications will be covered at a copay with the deductible waived. The Preventive Rx List can be found at
Summit BHC—EMB Beneits.
Deductibles and out-of-pocket maximums are embedded. If you enroll in employee + dependent(s) coverage, the individual deductible and out-of-
pocket applies to each covered member until the family limit is met.
4
BlueCross BlueShield of Tennessee
You have the highest level of coverage when visiting in-network providers.
z High Deductible Health Plan: allows you to pay less in premiums and you pay for the full cost of your doctor visits,
medical services and prescriptions, unless services or prescriptions are considered preventive. You can use a Health Savings
Account which provide a safety net for unexpected medical costs and tax advantages.
z PPO Plan: you will pay more in premiums and be responsible for paying copayments for doctor oice visits and
prescriptions. The deductible and 20% coinsurance will apply for all other services unless medical services are considered
preventive.
High Deductible Health Plan (HDHP) PPO Plan
In-Network In-Network
Calendar Year Deductible (embedded)
Individual $3,500 $2,500
Family $7,000 $6,000
Annual Out-of-Pocket Maximum (includes deductible)
Individual $6,000 $6,000
Family $12,000 $12,000
Oice Visits
Preventive Services Covered at 100% Covered at 100%
Telehealth Visit 20% after deductible up to $45 $10 per visit
Primary Care Physician 20% after deductible $35 copay
Specialist Oice Visit 20% after deductible $60 copay
Urgent Care 20% after deductible $60 copay
Hospital
Inpatient 20% after deductible 20% after deductible
Outpatient 20% after deductible 20% after deductible
Emergency Room 20% after deductible $250 copay plus 20% after deductible
Prescription Drugs
Preventive Drugs $5/$25/$50 deductible waived* Not applicable
Retail (30-day supply)
Tier 1 20% after deductible $10 copay
Tier 2 20% after deductible $75 copay
Tier 3 20% after deductible $150 copay
Mail Order (90-day supply)
Tier 1 20% after deductible $30 copay
Tier 2 20% after deductible $225 copay
Tier 3 20% after deductible $450 copay
Please note: The above chart shows your medical plan beneits for in-network coverage only. Your plan ofers out-of-network beneits; however,
beneits are reduced when care is provided out-of-network. For details and the terms of your medical and pharmacy plan beneits, refer to your
Certiicate of Insurance. If there are any inconsistencies between this summary and the oicial plan document/certiicates of coverage, the plan
document/certiicates of coverage will prevail.
* Preventive medications will be covered at a copay with the deductible waived. The Preventive Rx List can be found at
Summit BHC—EMB Beneits.
Deductibles and out-of-pocket maximums are embedded. If you enroll in employee + dependent(s) coverage, the individual deductible and out-of-
pocket applies to each covered member until the family limit is met.
4