
Page 17 - 2022 AEO Benefit Guide
P. 17
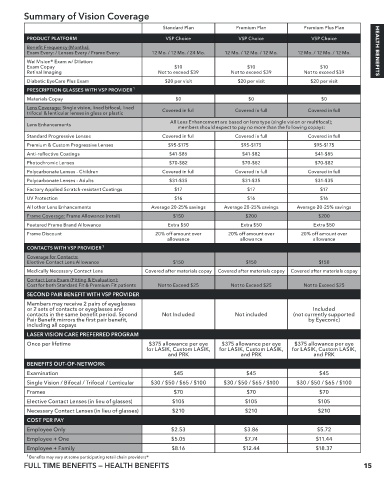
Summary of Vision Coverage
Standard Plan Premium Plan Premium Plus Plan
PRODUCT PLATFORM VSP Choice VSP Choice VSP Choice
Benefit Frequency (Months):
Exam Every: / Lenses Every / Frame Every: 12 Mo. / 12 Mo. / 24 Mo. 12 Mo. / 12 Mo. / 12 Mo. 12 Mo. / 12 Mo. / 12 Mo. HEALTH BENEFITS
WellVision® Exam w/ Dilation:
Exam Copay $10 $10 $10
Retinal Imaging Not to exceed $39 Not to exceed $39 Not to exceed $39
Diabetic EyeCare Plus Exam $20 per visit $20 per visit $20 per visit
PRESCRIPTION GLASSES WITH VSP PROVIDER 1
Materials Copay $0 $0 $0
Lens Coverage: Single vision, lined bifocal, lined Covered in full Covered in full Covered in full
trifocal & lenticular lenses in glass or plastic
All Lens Enhancement are based on lens type (single vision or multifocal);
Lens Enhancements
members should expect to pay no more than the following copays:
Standard Progressive Lenses Covered in full Covered in full Covered in full
Premium & Custom Progressive Lenses $95-$175 $95-$175 $95-$175
Anti-reflective Coatings $41-$85 $41-$82 $41-$85
Photochromic Lenses $70-$82 $70-$82 $70-$82
Polycarbonate Lenses - Children Covered in full Covered in full Covered in full
Polycarbonate Lenses - Adults $31-$35 $31-$35 $31-$35
Factory Applied Scratch-resistant Coatings $17 $17 $17
UV Protection $16 $16 $16
All other Lens Enhancements Average 20-25% savings Average 20-25% savings Average 20-25% savings
Frame Coverage: Frame Allowance (retail) $150 $200 $200
Featured Frame Brand Allowance Extra $50 Extra $50 Extra $50
Frame Discount 20% off amount over 20% off amount over 20% off amount over
allowance allowance allowance
CONTACTS WITH VSP PROVIDER 1
Coverage for Contacts:
Elective Contact Lens Allowance $150 $150 $150
Medically Necessary Contact Lens Covered after materials copay Covered after materials copay Covered after materials copay
Contact Lens Exam (Fitting & Evaluation):
Cost for both Standard Fit & Premium Fit patients Not to Exceed $25 Not to Exceed $25 Not to Exceed $25
SECOND PAIR BENEFIT WITH VSP PROVIDER
Members may receive 2 pairs of eyeglasses
or 2 sets of contacts or eyeglasses and Included
contacts in the same benefit period. Second Not Included Not included (not currently supported
Pair Benefit mirrors the first pair benefit, by Eyeconic)
including all copays
LASER VISION CARE PREFERRED PROGRAM
Once per lifetime $375 allowance per eye $375 allowance per eye $375 allowance per eye
for LASIK, Custom LASIK, for LASIK, Custom LASIK, for LASIK, Custom LASIK,
and PRK and PRK and PRK
BENEFITS OUT-OF-NETWORK
Examination $45 $45 $45
Single Vision / Bifocal / Trifocal / Lenticular $30 / $50 / $65 / $100 $30 / $50 / $65 / $100 $30 / $50 / $65 / $100
Frames $70 $70 $70
Elective Contact Lenses (in lieu of glasses) $105 $105 $105
Necessary Contact Lenses (in lieu of glasses) $210 $210 $210
COST PER PAY
Employee Only $2.53 $3.86 $5.72
Employee + One $5.05 $7.74 $11.44
Employee + Family $8.16 $12.44 $18.37
1 Benefits may vary at some participating retail chain providers®
FULL TIME BENEFITS — HEALTH BENEFITS 15