
Page 6 - 2022 US Benefits Guide FINAL
P. 6
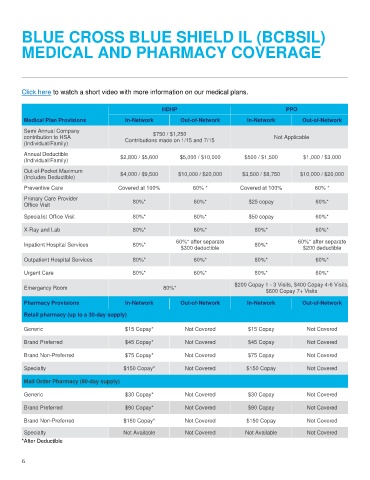
BLUE CROSS BLUE SHIELD IL (BCBSIL)
MEDICAL AND PHARMACY COVERAGE
Click here to watch a short video with more information on our medical plans.
HDHP PPO
Medical Plan Provisions In-Network Out-of-Network In-Network Out-of-Network
Semi Annual Company $750 / $1,250
contribution to HSA Contributions made on 1/15 and 7/15 Not Applicable
(Individual/Family)
Annual Deductible $2,800 / $5,600 $5,000 / $10,000 $500 / $1,500 $1,000 / $3,000
(Individual/Family)
Out-of-Pocket Maximum
$4,000 / $9,500 $10,000 / $20,000 $3,500 / $8,750 $10,000 / $20,000
(Includes Deductible)
Preventive Care Covered at 100% 60% * Covered at 100% 60% *
Primary Care Provider 80%* 60%* $25 copay 60%*
Office Visit
Specialist Office Visit 80%* 60%* $50 copay 60%*
X-Ray and Lab 80%* 60%* 80%* 60%*
60%* after separate 60%* after separate
Inpatient Hospital Services 80%* 80%*
$300 deductible $200 deductible
Outpatient Hospital Services 80%* 60%* 80%* 60%*
Urgent Care 80%* 60%* 80%* 60%*
$200 Copay 1 - 3 Visits, $400 Copay 4-6 Visits,
Emergency Room 80%*
$600 Copay 7+ Visits
Pharmacy Provisions In-Network Out-of-Network In-Network Out-of-Network
Retail pharmacy (up to a 30-day supply)
Generic $15 Copay* Not Covered $15 Copay Not Covered
Brand Preferred $45 Copay* Not Covered $45 Copay Not Covered
Brand Non-Preferred $75 Copay* Not Covered $75 Copay Not Covered
Specialty $150 Copay* Not Covered $150 Copay Not Covered
Mail Order Pharmacy (90-day supply)
Generic $30 Copay* Not Covered $30 Copay Not Covered
Brand Preferred $90 Copay* Not Covered $90 Copay Not Covered
Brand Non-Preferred $150 Copay* Not Covered $150 Copay Not Covered
Specialty Not Available Not Covered Not Available Not Covered
*After Deductible
6