
Page 7 - 2022 US Benefits Guide FINAL
P. 7
KAISER MEDICAL AND
PHARMACY COVERAGE
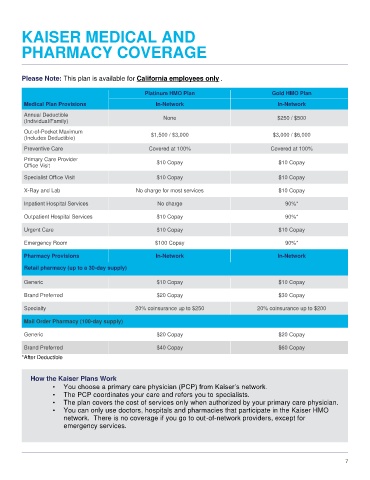
Please Note: This plan is available for California employees only .
Platinum HMO Plan Gold HMO Plan
Medical Plan Provisions In-Network In-Network
Annual Deductible
(Individual/Family) None $250 / $500
Out-of-Pocket Maximum $1,500 / $3,000 $3,000 / $6,000
(Includes Deductible)
Preventive Care Covered at 100% Covered at 100%
Primary Care Provider $10 Copay $10 Copay
Office Visit
Specialist Office Visit $10 Copay $10 Copay
X-Ray and Lab No charge for most services $10 Copay
Inpatient Hospital Services No charge 90%*
Outpatient Hospital Services $10 Copay 90%*
Urgent Care $10 Copay $10 Copay
Emergency Room $100 Copay 90%*
Pharmacy Provisions In-Network In-Network
Retail pharmacy (up to a 30-day supply)
Generic $10 Copay $10 Copay
Brand Preferred $20 Copay $30 Copay
Specialty 20% coinsurance up to $250 20% coinsurance up to $200
Mail Order Pharmacy (100-day supply)
Generic $20 Copay $20 Copay
Brand Preferred $40 Copay $60 Copay
*After Deductible
How the Kaiser Plans Work
• You choose a primary care physician (PCP) from Kaiser’s network.
• The PCP coordinates your care and refers you to specialists.
• The plan covers the cost of services only when authorized by your primary care physician.
• You can only use doctors, hospitals and pharmacies that participate in the Kaiser HMO
network. There is no coverage if you go to out-of-network providers, except for
emergency services.
7