
Page 18 - OpenX 2022 Book of Benefits
P. 18
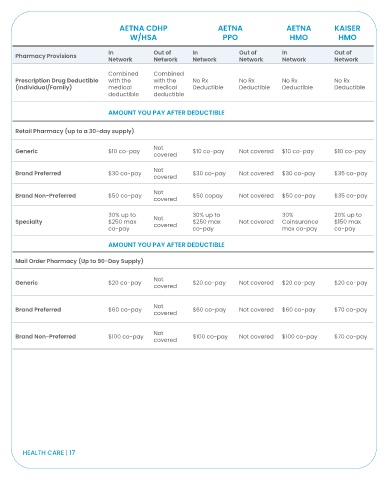
AETNA CDHP AETNA AETNA KAISER
W/HSA PPO HMO HMO
In Out of In Out of In Out of
Pharmacy Provisions
Network Network Network Network Network Network
Combined Combined
Prescription Drug Deductible with the with the No Rx No Rx No Rx No Rx
(Individual/Family) medical medical Deductible Deductible Deductible Deductible
deductible deductible
AMOUNT YOU PAY AFTER DEDUCTIBLE
Retail Pharmacy (up to a 30-day supply)
Not
Generic $10 co-pay $10 co-pay Not covered $10 co-pay $10 co-pay
covered
Not
Brand Preferred $30 co-pay $30 co-pay Not covered $30 co-pay $35 co-pay
covered
Not
Brand Non-Preferred $50 co-pay $50 copay Not covered $50 co-pay $35 co-pay
covered
30% up to 30% up to 30% 20% up to
Specialty $250 max Not $250 max Not covered Coinsurance $150 max
covered
co-pay co-pay max co-pay co-pay
AMOUNT YOU PAY AFTER DEDUCTIBLE
Mail Order Pharmacy (Up to 90-Day Supply)
Not
Generic $20 co-pay $20 co-pay Not covered $20 co-pay $20 co-pay
covered
Not
Brand Preferred $60 co-pay $60 co-pay Not covered $60 co-pay $70 co-pay
covered
Not
Brand Non-Preferred $100 co-pay $100 co-pay Not covered $100 co-pay $70 co-pay
covered
HEALTH CARE | 17