
Page 12 - Goodwill Columbus 2022 Benefit Guide
P. 12
A Guide to Your Benefits | 2022
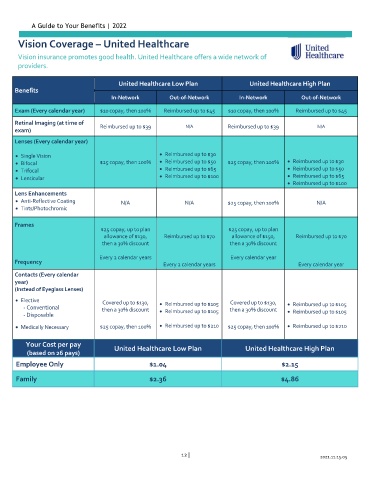
Vision Coverage – United Healthcare
Vision insurance promotes good health. United Healthcare offers a wide network of
providers.
United Healthcare Low Plan United Healthcare High Plan
Benefits
In-Network Out-of-Network In-Network Out-of-Network
Exam (Every calendar year) $10 copay, then 100% Reimbursed up to $45 $10 copay, then 100% Reimbursed up to $45
Retinal Imaging (at time of
Reimbursed up to $39 N/A Reimbursed up to $39 N/A
exam)
Lenses (Every calendar year)
Single Vision Reimbursed up to $30
Bifocal $25 copay, then 100% Reimbursed up to $50 $25 copay, then 100% Reimbursed up to $30
Trifocal Reimbursed up to $65 Reimbursed up to $50
Lenticular Reimbursed up to $100 Reimbursed up to $65
Reimbursed up to $100
Lens Enhancements
Anti-Reflective Coating N/A N/A $25 copay, then 100% N/A
Tints/Photochromic
Frames
$25 copay, up to plan $25 copay, up to plan
allowance of $130, Reimbursed up to $70 allowance of $150, Reimbursed up to $70
then a 30% discount then a 30% discount
Every 2 calendar years Every calendar year
Frequency Every 2 calendar years Every calendar year
Contacts (Every calendar
year)
(Instead of Eyeglass Lenses)
Elective
Covered up to $130, Reimbursed up to $105 Covered up to $130, Reimbursed up to $105
- Conventional
then a 30% discount Reimbursed up to $105 then a 30% discount Reimbursed up to $105
- Disposable
Medically Necessary $25 copay, then 100% Reimbursed up to $210 $25 copay, then 100% Reimbursed up to $210
Your Cost per pay United Healthcare Low Plan United Healthcare High Plan
(based on 26 pays)
Employee Only $1.04 $2.15
Family $2.36 $4.86
12 | 2021.11.15.05