
Page 14 - 2022 SoFi - August Open Enrollment
P. 14
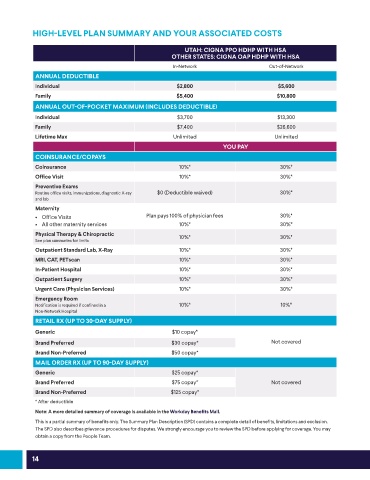
HIGH-LEVEL PLAN SUMMARY AND YOUR ASSOCIATED COSTS
UTAH: CIGNA PPO HDHP WITH HSA
OTHER STATES: CIGNA OAP HDHP WITH HSA
In-Network Out-of-Network
ANNUAL DEDUCTIBLE
Individual $2,800 $5,600
Family $5,400 $10,800
ANNUAL OUT-OF-POCKET MAXIMUM (INCLUDES DEDUCTIBLE)
Individual $3,700 $13,300
Family $7,400 $26,600
Lifetime Max Unlimited Unlimited
YOU PAY
COINSURANCE/COPAYS
Coinsurance 10%* 30%*
Office Visit 10%* 30%*
Preventive Exams
Routine office visits, immunizations, diagnostic X-ray $0 (Deductible waived) 30%*
and lab
Maternity
• Office Visits Plan pays 100% of physician fees 30%*
• All other maternity services 10%* 30%*
Physical Therapy & Chiropractic 10%* 30%*
See plan summaries for limits
Outpatient Standard Lab, X-Ray 10%* 30%*
MRI, CAT, PETscan 10%* 30%*
In-Patient Hospital 10%* 30%*
Outpatient Surgery 10%* 30%*
Urgent Care (Physician Services) 10%* 30%*
Emergency Room
Notification is required if confined in a 10%* 10%*
Non-Network Hospital
RETAIL RX (UP TO 30-DAY SUPPLY)
Generic $10 copay*
Brand Preferred $30 copay* Not covered
Brand Non-Preferred $50 copay*
MAIL ORDER RX (UP TO 90-DAY SUPPLY)
Generic $25 copay*
Brand Preferred $75 copay* Not covered
Brand Non-Preferred $125 copay*
* After deductible
Note: A more detailed summary of coverage is available in the Workday Benefits Mall.
This is a partial summary of benefits only. The Summary Plan Description (SPD) contains a complete detail of benefits, limitations and exclusion.
The SPD also describes grievance procedures for disputes. We strongly encourage you to review the SPD before applying for coverage. You may
obtain a copy from the People Team.
14