
Page 16 - 2022_Benefits_Book_Encharter_v9
P. 16
800-872-0500 i i 800-877-7195
deltadentalma.com vsp.com
Dental Plan Vision Plan
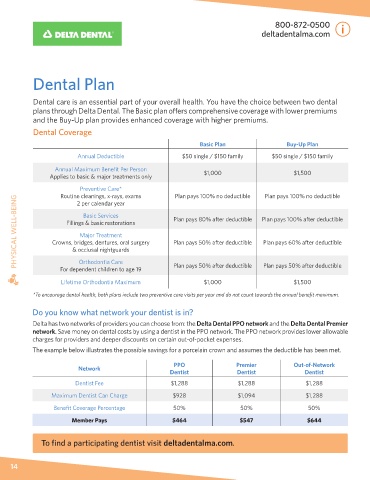
Dental care is an essential part of your overall health. You have the choice between two dental A routine eye exam is not only important for correcting vision, but can lead to the detection of
plans through Delta Dental. The Basic plan offers comprehensive coverage with lower premiums other serious health conditions. We offer employees and their dependents the choice between two
and the Buy-Up plan provides enhanced coverage with higher premiums. vision benefit plans through the Vision Service Plan (VSP).
Dental Coverage
IN-NETWORK Basic Plan Buy-Up Plan
Basic Plan Buy-Up Plan
Vision Exam
Annual Deductible $50 single / $150 family $50 single / $150 family (every calendar year) $10 Co-pay $10 Co-pay
Annual Maximum Benefit Per Person Prescription Glasses $20 Co-pay $20 Co-pay
Applies to basic & major treatments only $1,000 $1,500
Frames Plan pays up to $150 (every other calendar year) Plan pays up to $200 (every calendar year)
Preventive Care* Plan pays 100% no deductible Plan pays 100% no deductible Lenses Single, Bifocal, Trifocal Plan pays 100% (every calendar year) Plan pays 100% (every calendar year)
Routine cleanings, x-rays, exams
PHYSICAL WELL-BEING Crowns, bridges, dentures, oral surgery Plan pays 80% after deductible Plan pays 100% after deductible Standard $150–$175 Co-pay Up to $60 Co-pay PHYSICAL WELL-BEING
2 per calendar year
Progressive Lenses
$0 Co-pay
$0 Co-pay
Basic Services
Premium
$95–$105 Co-pay
$50 Co-pay
Fillings & basic restorations
$50 Co-pay
Custom
Major Treatment
Contacts Exam & Fitting
Up to $60 Co-pay
Plan pays 50% after deductible
Plan pays 60% after deductible
& occlusal nightguards
Prescription Contacts
(instead of glasses)
Orthodontia Care
Plan pays 50% after deductible
Plan pays 50% after deductible
For dependent children to age 19
Eye Care Visit Plan pays up to $150 (every calendar year) Plan pays up to $200 (every calendar year)
$20 Co-pay
$20 Co-pay
Lifetime Orthodontia Maximum $1,000 $1,500 Pink Eye, Eye Injury, Dry Eye
*To encourage dental health, both plans include two preventive care visits per year and do not count towards the annual benefit maximum.
Additional Discounts Available Through VSP Providers
Do you know what network your dentist is in? • 20% off of the cost of frames that exceeds your allowance.
Delta has two networks of providers you can choose from: the Delta Dental PPO network and the Delta Dental Premier • 20% savings on additional glasses and sunglasses, including lens enhancements, from any VSP provider within
network. Save money on dental costs by using a dentist in the PPO network. The PPO network provides lower allowable 12 months of your last WellVision Exam.
charges for providers and deeper discounts on certain out-of-pocket expenses. • Laser Vision Correction: Average 15% off the regular price or 5% off the promotional price (discounts only
The example below illustrates the possible savings for a porcelain crown and assumes the deductible has been met. available from contracted facilities).
Know Before You Go
PPO Premier Out-of-Network
Network
Dentist Dentist Dentist To take advantage of the vision plan hardware benefits, please be sure to go to an in-network provider. To find a
participating eye doctor and eyeglass store visit vsp.com.
Dentist Fee $1,288 $1,288 $1,288
Many eyeglass stores will mention that they are an out-of-network provider for VSP. This means you will pay full price for
Maximum Dentist Can Charge $928 $1,094 $1,288 glasses and will be required to submit a claim to VSP for reimbursement. Please note you will not receive the same level of
Benefit Coverage Percentage 50% 50% 50% benefits when the provider is out-of-network.
Member Pays $464 $547 $644 Primary Eye Care Program
If you have diabetic eye disease, glaucoma or age-related macular degeneration, you can receive your routine eye care
To find a participating dentist visit deltadentalma.com. and follow-up medical eye care services from your VSP doctor. You can also receive preventive retinal screenings if you
have diabetes, but don’t show signs of diabetic eye disease—services are covered with just a $20 co-pay per visit.
14 15