
Page 6 - VO 2021 Employee Benefits_No Notices
P. 6
Ventura Orthopedics
2021 Employee Benefits Brochure
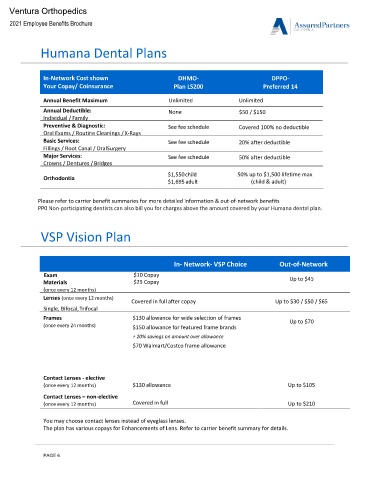
Humana Dental Plans
In-Network Cost shown DHMO- DPPO-
Your Copay/ Coinsurance Plan LS200 Preferred 14
Annual Benefit Maximum Unlimited Unlimited
Annual Deductible: None $50 / $150
Individual / Family
Preventive & Diagnostic: See fee schedule Covered 100% no deductible
Oral Exams / Routine Cleanings / X-Rays
Basic Services: See fee schedule 20% after deductible
Fillings / Root Canal / OralSurgery
Major Services: See fee schedule 50% after deductible
Crowns / Dentures / Bridges
$1,550 child 50% up to $1,500 lifetime max
Orthodontia
$1,695 adult (child & adult)
Please refer to carrier benefit summaries for more detailed information & out-of-network benefits
PP0 Non-participating dentists can also bill you for charges above the amount covered by your Humana dental plan.
VSP Vision Plan
In- Network- VSP Choice Out-of-Network
Exam $10 Copay
Materials $25 Copay Up to $45
(once every 12 months)
Lenses (once every 12 months)
Covered in full after copay Up to $30 / $50 / $65
Single, Bifocal, Trifocal
Frames $130 allowance for wide selection of frames Up to $70
(once every 24 months) $150 allowance for featured frame brands
+ 20% savings on amount over allowance
$70 Walmart/Costco frame allowance
Contact Lenses - elective
(once every 12 months) $130 allowance Up to $105
Contact Lenses – non-elective
(once every 12 months) Covered in full Up to $210
You may choose contact lenses instead of eyeglass lenses.
The plan has various copays for Enhancements of Lens. Refer to carrier benefit summary for details.
PAGE 6