
Page 29 - Binder - English for Doctors
P. 29
28
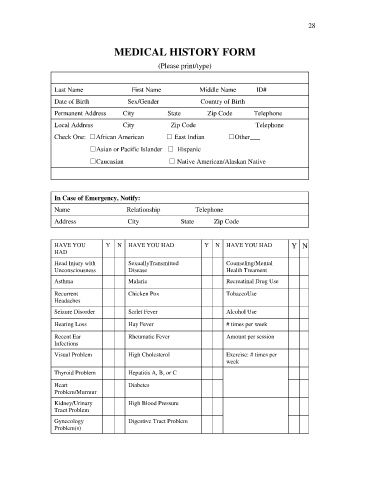
MEDICAL HISTORY FORM
(Please print/type)
Last Name First Name Middle Name ID#
Date of Birth Sex/Gender Country of Birth
Permanent Address City State Zip Code Telephone
Local Address City Zip Code Telephone
Check One: □African American □ East Indian □Other___
□Asian or Pacific Islander □ Hispanic
□Caucasian □ Native American/Alaskan Native
In Case of Emergency, Notify:
Name Relationship Telephone
Address City State Zip Code
HAVE YOU Y N HAVE YOU HAD Y N HAVE YOU HAD Y N
HAD
Head Injury with SexuallyTransmitted Counseling/Mental
Unconsciousness Disease Health Treament
Asthma Malaria Recreatinal Drug Use
Recurrent Chicken Pox TobaccoUse
Headaches
Seizure Disorder Scrlet Fever Alcohol Use
Hearing Loss Hay Fever # times per week
Recent Ear Rheumatic Fever Amount per session
Infections
Visual Problem High Cholesterol Exercise: # times per
week
Thyroid Problem Hepatitis A, B, or C
Heart Diabetes
Problem/Murmur
Kidney/Urinary High Blood Pressure
Tract Problem
Gynecology Digestive Tract Problem
Problem(s)