
Page 30 - Binder - English for Doctors
P. 30
29
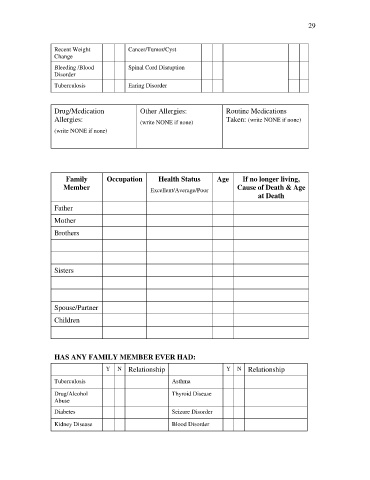
Recent Weight Cancer/Tumor/Cyst
Change
Bleeding /Blood Spinal Cord Disruption
Disorder
Tuberculosis Earing Disorder
Drug/Medication Other Allergies: Routine Medications
Allergies: (write NONE if none) Taken: (write NONE if none)
(write NONE if none)
Family Occupation Health Status Age If no longer living,
Member Excellent/Average/Poor Cause of Death & Age
at Death
Father
Mother
Brothers
Sisters
Spouse/Partner
Children
HAS ANY FAMILY MEMBER EVER HAD:
Y N Relationship Y N Relationship
Tuberculosis Asthma
Drug/Alcohol Thyroid Disease
Abuse
Diabetes Seizure Disorder
Kidney Disease Blood Disorder