
Page 44 - CASA Bulletin of Anesthesiology 2022; 9(3)-1 (1)
P. 44
CASA Bulletin of Anesthesiology
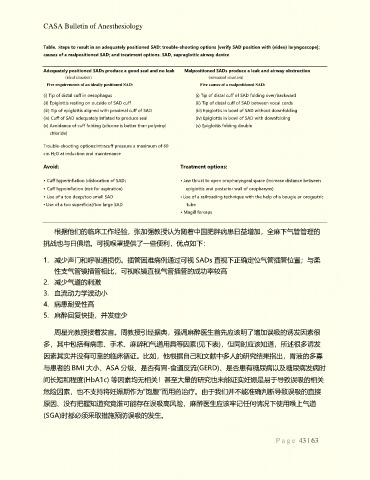
Table. Steps to result in an adequately positioned SAD; trouble-shooting options [verify SAD position with (video) laryngoscope];
causes of a malpositioned SAD; and treatment options. SAD, supraglottic airway device
Adequately positioned SADs produce a good seal and no leak Malpositioned SADs produce a leak and airway obstruction
(ideal situation) (unwanted situation)
Five requirements of an ideally positioned SAD: Five causes of a malpositioned SAD:
(i) Tip of distal cuff in oesophagus (i) Tip of distal cuff of SAD folding over/backward
(ii) Epiglottis resting on outside of SAD cuff (ii) Tip of distal cuff of SAD between vocal cords
(iii) Tip of epiglottis aligned with proximal cuff of SAD (iii) Epiglottis in bowl of SAD without downfolding
(iv) Cuff of SAD adequately inflated to produce seal (iv) Epiglottis in bowl of SAD with downfolding
(v) Avoidance of cuff folding (silicone is better than polyvinyl (v) Epiglottis folding double
chloride)
Trouble-shooting options:Intracuff pressure a maximum of 60
cm H2O at induction and maintenance
Avoid: Treatment options:
• Cuff hyperinflation (dislocation of SAD) • Jaw thrust to open oropharyngeal space (increase distance between
• Cuff hypoinflation (risk for aspiration) epiglottis and posterior wall of oropharynx)
• Use of a too deep/too small SAD • Use of a railroading technique with the help of a bougie or orogastric
• Use of a too superficial/too large SAD tube
• Magill forceps
根据他们的临床工作经验,张加强教授认为随着中国肥胖病患日益增加,全麻下气管管理的
挑战也与日俱增。可视喉罩提供了一些便利,优点如下:
1. 减少声门和呼吸道损伤。插管困难病例通过可视 SADs 直视下正确定位气管插管位置;与柔
性支气管镜插管相比,可视喉镜直视气管插管的成功率较高
2. 减少气道的刺激
3. 血流动力学波动小
4. 病患耐受性高
5. 麻醉回复快捷,并发症少
周星光教授接着发言。周教授引经据典,强调麻醉医生首先应该明了增加误吸的诱发因素很
多,其中包括有病患、手术、麻醉和气道用具等因素(见下表),但同时应该知道,所述很多诱发
因素其实并没有可靠的临床循证。比如,他根据自己和文献中多人的研究结果指出,胃液的多寡
与患者的 BMI 大小、ASA 分级、是否有胃-食道反流(GERD)、是否患有糖尿病以及糖尿病发病时
间长短和程度(HbA1c) 等因素均无相关!甚至大量的研究也未能证实妊娠是易于导致误吸的相关
危险因素,也不支持将妊娠期作为“饱腹”而用药治疗。由于我们并不能准确判断导致误吸的直接
原因、没有把握知道究竟谁可能存在误吸高风险,麻醉医生应该牢记任何情况下使用喉上气道
(SGA)时都必须釆取措施预防误吸的发生。
P a g e 43 | 63