
Page 3 - Luminex 2018 Be Healthy 12pg with Notices v4_Neat
P. 3
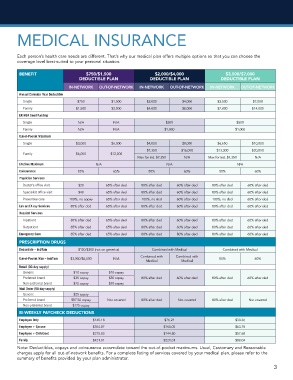
MEDICAL INSURANCE
Each person’s health care needs are different. That’s why our medical plan offers multiple options so that you can choose the
coverage level best-suited to your personal situation.
BENEFIT $750/$1,500 $2,000/$4,000 $3,500/$7,000
DEDUCTIBLE PLAN DEDUCTIBLE PLAN DEDUCTIBLE PLAN
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Annual Calendar Year Deductible
Single $750 $1,500 $2,000 $4,000 $3,500 $7,000
Family $1,500 $3,000 $4,000 $8,000 $7,000 $14,000
ER HSA Seed Funding
Single N/A N/A $500 $500
Family N/A N/A $1,000 $1,000
Out-of-Pocket Maximum
Single $3,000 $6,000 $4,000 $8,000 $6,650 $10,000
$7,350 $16,000 $13,300 $20,000
Family $6,000 $12,000
Max for ind. $7,350 N/A Max for ind. $7,350 N/A
Lifetime Maximum N/A N/A N/A
Coinsurance 85% 65% 80% 60% 80% 60%
Physician Services
Doctor’s office visit $20 65% after ded 80% after ded 60% after ded 80% after ded 60% after ded
Specialist office visit $40 65% after ded 80% after ded 60% after ded 80% after ded 60% after ded
Preventive care 100%, no copay 65% after ded 100%, no ded 60% after ded 100%, no ded 60% after ded
Lab and X-ray Services 85% after ded 65% after ded 80% after ded 60% after ded 80% after ded 60% after ded
Hospital Services
Inpatient 85% after ded 65% after ded 80% after ded 60% after ded 80% after ded 60% after ded
Outpatient 85% after ded 65% after ded 80% after ded 60% after ded 80% after ded 60% after ded
Emergency Care 85% after ded 65% after ded 80% after ded 80% after ded 80% after ded 60% after ded
PRESCRIPTION DRUGS
Deductible – Ind/Fam $100/$300 (not on generics) Combined with Medical Combined with Medical
Combined with Combined with
Out-of-Pocket Max – Ind/Fam $3,000/$6,000 N/A 80% 60%
Medical Medical
Retail (30-day supply)
Generic $10 copay $10 copay
Preferred brand $35 copay $35 copay 80% after ded 60% after ded 80% after ded 60% after ded
Non-preferred brand $70 copay $70 copay
Mail Order (90-day supply)
Generic $25 copay
Preferred brand $87.50 copay Not covered 80% after ded Not covered 80% after ded Not covered
Non-preferred brand $175 copay
BI-WEEKLY PAYCHECK DEDUCTIONS
Employee Only $145.18 $76.21 $30.36
Employee + Spouse $304.87 $160.05 $63.75
Employee + Child(ren) $275.83 $144.80 $57.68
Family $421.01 $221.01 $88.04
Note: Deductibles, copays and coinsurance accumulate toward the out-of-pocket maximums. Usual, Customary and Reasonable
charges apply for all out-of-network benefits. For a complete listing of services covered by your medical plan, please refer to the
summary of benefits provided by your plan administrator.
3