
Page 4 - Luminex 2018 Be Healthy 12pg with Notices v4_Neat
P. 4
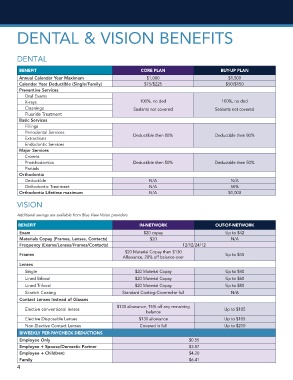
DENTAL & VISION BENEFITS
DENTAL
BENEFIT CORE PLAN BUY-UP PLAN
Annual Calendar Year Maximum $1,000 $1,500
Calendar Year Deductible (Single/Family) $75/$225 $50/$150
Preventive Services
Oral Exams
X-rays 100%, no ded 100%, no ded
Cleanings Sealants not covered Sealants not covered
Fluoride Treatment
Basic Services
Fillings
Periodontal Services
Extractions Deductible then 80% Deductible then 80%
Endodontic Services
Major Services
Crowns
Prosthodontics Deductible then 50% Deductible then 50%
Partials
Orthodontia
Deductible N/A N/A
Orthodontic Treatment N/A 50%
Orthodontia Lifetime maximum N/A $1,000
VISION
Additional savings are available from Blue View Vision providers
BENEFIT IN-NETWORK OUT-OF-NETWORK
Exam $20 copay Up to $42
Materials Copay (Frames, Lenses, Contacts) $20 N/A
Frequency (Exams/Lenses/Frames/Contacts) 12/12/24/12
$20 Material Copay then $130
Frames Up to $45
Allowance, 20% off balance over
Lenses
Single $20 Material Copay Up to $40
Lined Bifocal $20 Material Copay Up to $60
Lined Trifocal $20 Material Copay Up to $80
Scratch Coating Standard Coating Covered-in-full N/A
Contact Lenses Instead of Glasses
$130 allowance, 15% off any remaining
Elective conventional lenses Up to $105
balance
Elective Disposable Lenses $130 allowance Up to $105
Non-Elective Contact Lenses Covered in full Up to $210
BIWEEKLY PER-PAYCHECK DEDUCTIONS
Employee Only $0.55
Employee + Spouse/Domestic Partner $3.87
Employee + Child(ren) $4.20
Family $6.41
4