
Page 9 - 3z.20 Employee Benefits
P. 9
to see a specialist?
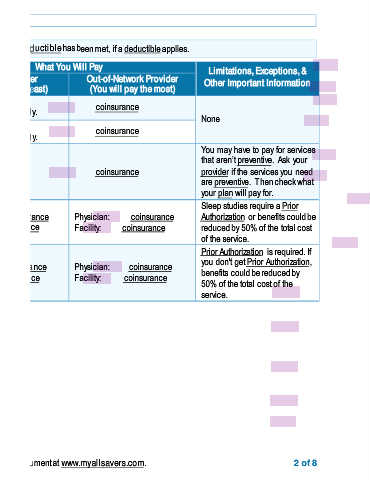
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.
Common What You Will Pay Limitations, Exceptions, &
Medical Event Services You May Need Network Provider Out-of-Network Provider Other Important Information
(You will pay the least) (You will pay the most)
Primary care visit to treat an copay/visit coinsurance
injury or illness Deductible does not apply. None
If you visit a health Specialist visit copay/visit coinsurance
Deductible does not apply.
care provider’s office You may have to pay for services
or clinic that aren’t preventive. Ask your
Preventive care/screening/ No charge coinsurance provider if the services you need
immunization
are preventive. Then check what
your plan will pay for.
Sleep studies require a Prior
Diagnostic test (x-ray, blood Physician: coinsurance Physician: coinsurance Authorization or benefits could be
work) Facility: coinsurance Facility: coinsurance reduced by 50% of the total cost
of the service.
If you have a test Prior Authorization is required. If
Imaging (CT/PET scans, Physician: coinsurance Physician: coinsurance you don't get Prior Authorization,
benefits could be reduced by
MRIs) Facility: coinsurance Facility: coinsurance
50% of the total cost of the
service.
* For more information about limitations and exceptions, see the plan or policy document at www.myallsavers.com. 2 of 8