
Page 13 - 3z.20 Employee Benefits
P. 13
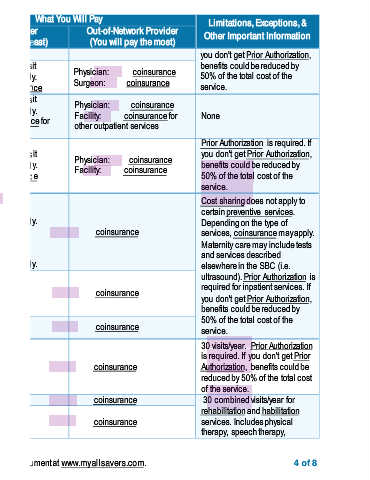
Common What You Will Pay Limitations, Exceptions, &
Medical Event Services You May Need Network Provider Out-of-Network Provider Other Important Information
(You will pay the least) (You will pay the most)
stay room) you don't get Prior Authorization,
Physician: copay/visit benefits could be reduced by
Physician/surgeon fees Deductible does not apply. Physician: coinsurance 50% of the total cost of the
Surgeon: coinsurance Surgeon: coinsurance service.
Physician: copay/visit Physician: coinsurance
Outpatient services Deductible does not apply. Facility: coinsurance for None
If you need mental Facility: coinsurance for other outpatient services
other outpatient services
health, behavioral Prior Authorization is required. If
health, or substance Physician: copay/visit you don't get Prior Authorization,
abuse services Physician: coinsurance
Inpatient services Deductible does not apply. Facility: coinsurance benefits could be reduced by
Facility: coinsurance 50% of the total cost of the
service.
Primary Care Visit: Cost sharing does not apply to
copay/visit* certain preventive services.
Deductible does not apply. Depending on the type of
Office visits coinsurance services, coinsurance may apply.
Specialist Visit: Maternity care may include tests
copay/visit* and services described
If you are pregnant Deductible does not apply. elsewhere in the SBC (i.e.
ultrasound). Prior Authorization is
Childbirth/delivery required for inpatient services. If
professional services coinsurance coinsurance you don't get Prior Authorization,
benefits could be reduced by
Childbirth/delivery facility coinsurance coinsurance 50% of the total cost of the
services service.
30 visits/year. Prior Authorization
is required. If you don't get Prior
Home health care coinsurance coinsurance Authorization, benefits could be
If you need help reduced by 50% of the total cost
recovering or have of the service.
other special health
needs Rehabilitation services coinsurance coinsurance 30 combined visits/year for
rehabilitation and habilitation
Habilitation services coinsurance coinsurance services. Includes physical
therapy, speech therapy,
* For more information about limitations and exceptions, see the plan or policy document at www.myallsavers.com. 4 of 8