
Page 10 - 3z.20 Employee Benefits
P. 10
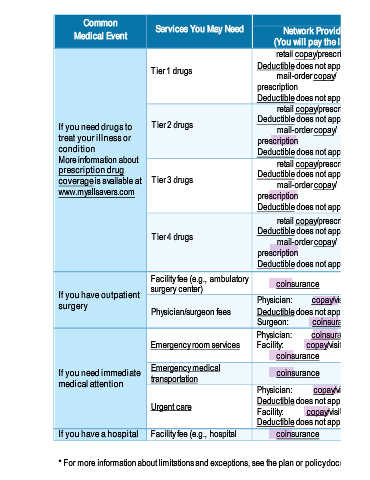
Common What You Will Pay Limitations, Exceptions, &
Medical Event Services You May Need Network Provider Out-of-Network Provider Other Important Information
(You will pay the least) (You will pay the most)
retail copay/prescription, or retail copay/prescription, or
Tier 1 drugs Deductible does not apply. Deductible does not apply.
mail-order copay/
mail-order copay/
prescription prescription Covers up to a 30-day supply
(retail subscription); 31-90 day
Deductible does not apply. Deductible does not apply. supply (mail prescription).
retail copay/prescription, or retail copay/prescription, or If a dispensed drug has a
Deductible does not apply. Deductible does not apply. chemically equivalent drug at a
If you need drugs to Tier 2 drugs mail-order copay/ mail-order copay/
treat your illness or prescription prescription lower tier, the cost difference
between drugs in addition to any
condition Deductible does not apply. eductible does not apply. applicable copay and/or
D
More information about retail copay/prescription, or retail copay/prescription, or coinsurance may be applied.
prescription drug Deductible does not apply. Deductible does not apply.
coverage is available at Tier 3 drugs mail-order copay/ mail-order copay/ Certain drugs may have a prior
authorization requirement.
www.myallsavers.com prescription prescription If you use an out-of-network
D
Deductible does not apply. eductible does not apply. pharmacy (including a mail order
retail copay/prescription, or retail copay/prescription, or pharmacy), you may be
Deductible does not apply. Deductible does not apply. responsible for any amount over
Tier 4 drugs mail-order copay/ mail-order copay/ the allowed amount.
prescription prescription
D
Deductible does not apply. eductible does not apply.
Facility fee (e.g., ambulatory Prior Authorization is required. If
surgery center) coinsurance coinsurance you don't get Prior Authorization,
If you have outpatient Physician: copay/visit benefits could be reduced by
surgery Physician: coinsurance
Physician/surgeon fees Deductible does not apply. Surgeon: coinsurance 50% of the total cost of the
Surgeon: coinsurance service.
Physician: coinsurance Physician: coinsurance*
Emergency room services Facility: copay/visit and Facility: copay/visit and *Out-of-network emergency
coinsurance coinsurance* services are covered at the
Emergency medical Network benefit level.
If you need immediate transportation coinsurance coinsurance*
medical attention
Physician: copay/visit
Deductible does not apply. Physician: coinsurance One copay is applied per network
Urgent care Facility: copay/visit Facility: coinsurance urgent care visit.
Deductible does not apply.
If you have a hospital Facility fee (e.g., hospital coinsurance coinsurance Prior Authorization is required. If
* For more information about limitations and exceptions, see the plan or policy document at www.myallsavers.com. 3 of 8