
Page 110 - Veterinary Laser Therapy in Small Animal Practice
P. 110
96 Veterinary Laser Therapy in Small Animal Practice
Case no. 11
G., feline, 5 years old, Domestic Shorthair, MC, 5.5 kg
• Complaint: wound, skin progressively coming off.
• History: G. disappeared for a couple of days and came home with his rear end covered in what seemed to be
motor oil. Owners noticed skin in that area started to first harden and then come off.
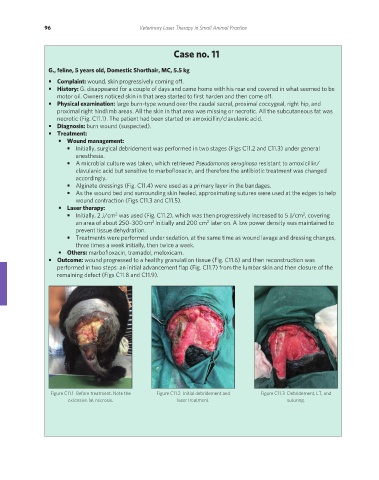
• Physical examination: large burn-type wound over the caudal sacral, proximal coccygeal, right hip, and
proximal right hindlimb areas. All the skin in that area was missing or necrotic. All the subcutaneous fat was
necrotic (Fig. C11.1). The patient had been started on amoxicillin/clavulanic acid.
• Diagnosis: burn wound (suspected).
• Treatment:
• Wound management:
• Initially, surgical debridement was performed in two stages (Figs C11.2 and C11.3) under general
anesthesia.
• A microbial culture was taken, which retrieved Pseudomonas aeruginosa resistant to amoxicillin/
clavulanic acid but sensitive to marbofloxacin, and therefore the antibiotic treatment was changed
accordingly.
• Alginate dressings (Fig. C11.4) were used as a primary layer in the bandages.
• As the wound bed and surrounding skin healed, approximating sutures were used at the edges to help
wound contraction (Figs C11.3 and C11.5).
• Laser therapy:
2
2
• Initially, 2 J/cm was used (Fig. C11.2), which was then progressively increased to 5 J/cm , covering
2
2
an area of about 250–300 cm initially and 200 cm later on. A low power density was maintained to
prevent tissue dehydration.
• Treatments were performed under sedation, at the same time as wound lavage and dressing changes,
three times a week initially, then twice a week.
• Others: marbofloxacin, tramadol, meloxicam.
• Outcome: wound progressed to a healthy granulation tissue (Fig. C11.6) and then reconstruction was
performed in two steps: an initial advancement flap (Fig. C11.7) from the lumbar skin and then closure of the
remaining defect (Figs C11.8 and C11.9).
Figure C11.1 Before treatment. Note the Figure C11.2 Initial debridement and Figure C11.3 Debridement, LT, and
extensive fat necrosis. laser treatment. suturing.
REDONDO PRINT (4-COL BLEED).indd 96 08/08/2019 09:48