
Page 6 - GP Spring 2024
P. 6
After making mucogingival incisions on the zygoma along the mesial wall of the maxillary
sinus, above the maxillary right and left first molars, the surgeon inserts the miniplate or
miniscrew on the zygomatic buttress (Figure 1). Immediate force loading is applied with power
Miniplates or Miniscrews as a Cervical Headgear Alternative for
threat, power chain or nickel titanium coils attached from the skeletal anchorage and connected
to a hook crimped between the canine and the lateral incisor on a cinched maxillary heavy
Orthopedic Correction of Class II Skeletal and Dental Non-compliant
rectangular stainless arch wire. This system controls and directs the growth of the maxillary arch
Growing Patients and dentition distally allowing the mandible to “catch” with the differential growth. In this
manner, a class I is achieved without moving the dental dentition anteriorly compromising the
periodontium and the stability. 6
Author: AnaMaria Munoz, DDS, MS
Despite poor patient cooperation, all the original treatment objectives of these two cases were
achieved. The facial harmony and lip support were improved, 10,11 the smile was made more
This article describes the use of minplates/ has shown no negative effects. However, esthetic by broadening the maxillary and mandibular arches, and Class I canine and molar
7
miniscrews inserted in the zygomatic but- cooperation is crucial for the success of the relationships were produced on both sides (Figures 2-5).
tress for skeletal anchorage in a growing treatment. As Xavier Casas Estivales from
adolescent patient with a class II division Spain says, “Currently our main problem is In these cases, skeletal anchorage at the zygoma above the maxillary molars proved a good
alternative to the initial cervical headgear therapy, which was hindered by poor patient
1 malocclusion as an alternative treatment the patient cooperation, we face a society cooperation.
when the patient is not cooperating with a where effort is not a value, and we have to
headgear. 1 replace it with imagination and innovative
clinical resources to be successful.” 8
Approximately 50-60% of orthodontic pa-
tients have a class II division 1 malocclu- This article describes the use of miniplates/
sion. These may involve anterior-posterior miniscrews inserted in the zygomatic but-
skeletal discrepancies such as a protruding tress for skeletal anchorage in a growing
9
maxilla or a retrognathic mandible, reflect- adolescent patient with a class II division Figure 1. Anatomical location of the skele-
ing a convex profile. If the maxilla is prog- 1 malocclusion when the patient is not co- tal anchorage (minplates/miniscrews).
Figure 1. Anatomical location of the skeletal anchorage (minplates/miniscrews).
nathic, it is desirable to retrude it. There is operating with the headgear therapy despite
evidence to suggest that this is indeed pos- the motivational efforts after nine months to
sible. Forces applied to the maxilla during a year of treatment.
active growth, directing it distally, are ap-
parently capable of growth restraint and/or After making mucogingival incisions on
redirection. Presumably this force at least the zygoma along the mesial wall of the
may redirect the forward growing maxilla maxillary sinus, above the maxillary right
to grow vertically. The mandible, which and left first molars, the surgeon inserts the
may be growing at a faster rate (differential miniplate or miniscrew on the zygomatic
growth) will then “catch up” to the maxil- buttress (Figure 1). Immediate force load-
la, aligning the bony bases. A similar ap- ing is applied with power threat, power
proach is followed even when the mandible chain or nickel titanium coils attached from
is retrognathic and the maxilla is correctly the skeletal anchorage and connected to a
positioned, because of the apparent limited hook crimped between the canine and the
ability to stimulate the mandible to grow. lateral incisor on a cinched maxillary heavy
The aim of this procedure is to establish har- rectangular stainless arch wire. This system
mony between the apical bases even though controls and directs the growth of the max-
they may both be related retrognathically illary arch and dentition distally allowing
to the face because facial imbalance is less the mandible to “catch” with the differential
notable when the apical bases (ANB angle) growth. In this manner, a class I is achieved
are in harmony. Therefore, it constitutes a without moving the dental dentition ante-
suitable compromise. (A mandible which is riorly compromising the periodontium and
excessively retrognathic may require sur- the stability. 6
gery). 2
Despite poor patient cooperation, all the
Studies show that the success rate using original treatment objectives of these two
headgear is 81% while functional applianc- cases were achieved. The facial harmony
es it is only 56%. 3,4 The cervical headgear and lip support were improved, 10,11 the smile
is not only the most efficient and predictable was made more esthetic by broadening the
orthopedic appliance to correct a class II maxillary and mandibular arches, and Class
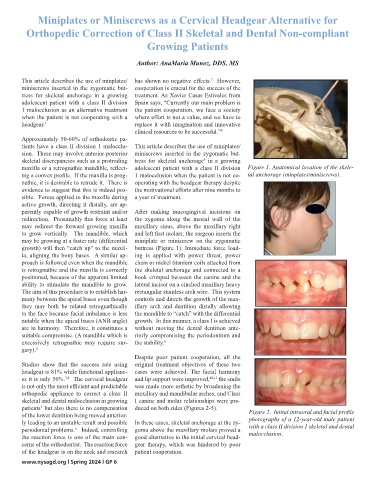
skeletal and dental malocclusion in growing I canine and molar relationships were pro-
patients but also there is no compensation duced on both sides (Figures 2-5).
5
of the lower dentition being moved anterior- Figure 2. Initial intraoral and facial profile
ly leading to an unstable result and possible In these cases, skeletal anchorage at the zy- photographs of a 12-year-old male patient
periodontal problems. Indeed, controlling goma above the maxillary molars proved a with a class II division 1 skeletal and dental
6
the reaction force is one of the main con- good alternative to the initial cervical head- malocclusion.
cerns of the orthodontist. The reaction force gear therapy, which was hindered by poor
of the headgear is on the neck and research patient cooperation.
www.nysagd.org l Spring 2024 l GP 6