
Page 271 - fourth year book
P. 271
DIABETES MELLITUS
hyperglycemia and ketosis; therefore vigorous activity should be
avoided in the presence of ketosis.
Hypoglycemia: in individual taking insulin and/or insulin
secratagogues, physical activity can cause hypoglycemia if
carbohydrates consumption is not adequate. So, added
carbohydrates should be ingested if pre-exercise glucose levels are
< 100 mg/dl.
Exercise in presence of long-term complication of diabetes:
Retinopathy: in the presence of severe proliferative diabetic
retinopathy , severe or vigorous aerobic or resistance exercise may
be contraindicated because the risk of trigging vitreous
hemorrhage or retinal detachment
Peripheral neuropathy: in the presence of severe neuropathy, it
may be best to encourage non-weight-bearing activities such as
swimming, bicycling or arm exercise.
Albuminuria and nephropathy: physical activity can acutely
increase urinary protein excretion. However, there is no evidence
that vigorous exercise increase the rate of progression of diabetic
kidney disease so there is no need for specific exercise restrictions
for people with diabetic kidney disease.
2) Pharmacologic management of diabetes.
a) Oral hypoglycemic drugs:
Oral hypoglycemic drugs are used in treating persons with type 2
diabetes who are controlled by diet and exercise.
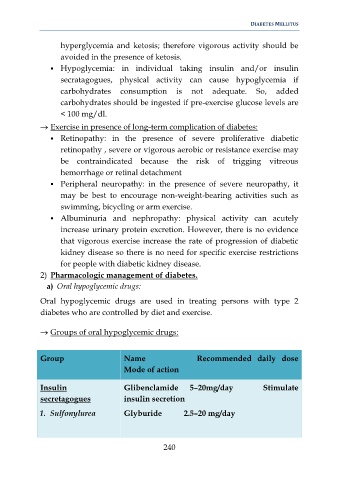
Groups of oral hypoglycemic drugs:
Group Name Recommended daily dose
Mode of action
Insulin Glibenclamide 5–20mg/day Stimulate
secretagogues insulin secretion
1. Sulfonylurea Glyburide 2.5–20 mg/day
240