
Page 30 - CJO_F17_GLAUCOMA_SUPPLEMENT
P. 30
C CLINICAL RESEARCH
ness in the mid-70s or an inter-eye asymmetry of 6 to 9μm is considered suspicious. 241,242
It is also critical to recognize that localized RNFL loss may not significantly impact global thickness
(as noted in Figure 10), but can lead to substantial focal VF loss. That being said, in the absence of a
243
definite structure-function correlation, any localized RNFL thinning must be confirmed, as quadrant and
clock hour measurements have relatively poor reproducibility as compared to global (average) param-
eters. The RNFL profile indicating the characteristic “double hump” pattern is a good place to look to
244
identify localized RNFL thinning (as noted in Figure 10).
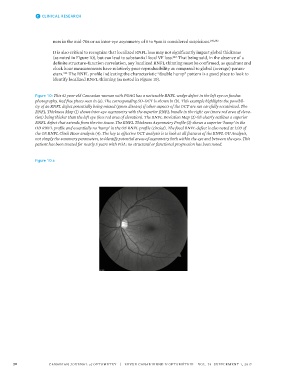
Figure 10: This 61 year-old Caucasian woman with POAG has a noticeable RNFL wedge defect in the left eye on fundus
photography. Red free photo seen in (a). The corresponding SD-OCT is shown in (b). This example highlights the possibil-
ity of an RNFL defect potentially being missed (green disease) if other aspects of the OCT are not carefully scrutinized. The
RNFL Thickness Map (1) shows inter-eye asymmetry with the superior RNFL bundle in the right eye (more red area of eleva-
tion) being thicker than the left eye (less red area of elevation). The RNFL Deviation Map (2) OS clearly outlines a superior
RNFL defect that extends from the rim tissue. The RNFL Thickness Asymmetry Profile (3) shows a superior ‘hump’ in the
OD RNFL profile and essentially no ‘hump’ in the OS RNFL profile (circled). The focal RNFL defect is also noted at 1:00 of
the OS RNFL Clock Hour analysis (4). The key to effective OCT analysis is to look at all features of the RNFL OU Analysis,
not simply the summary parameters, to identify potential areas of asymmetry both within the eye and between the eyes. This
patient has been treated for nearly 5 years with PGA: no structural or functional progression has been noted.
Figure 10 a
30 CANADIAN JOURNAL of OPTOMETRY | REVUE CANADIENNE D’OPTOMÉTRIE VOL. 79 SUPPLEMENT 1, 2017