Page 5 - 2019 CareHere Enrollment Guide
P. 5
CAREHERE
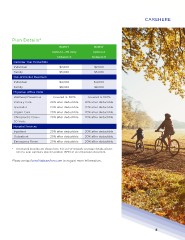
Plan Details*
BCBST BCBST
Option 1—TN Only Option 2
Network S Network P
Calendar Year Deductible
Individual $2,600 $2,600
Family $5,000 $5,000
Out-of-Pocket Maximum
Individual $4,000 $4,000
Family $8,000 $8,000
Physician Office Visits
Wellness/Preventive Covered at 100% Covered at 100%
Primary Care 20% after deductible 20% after deductible
Specialist 20% after deductible 20% after deductible
Urgent Care 20% after deductible 20% after deductible
Chiropractic Care— 20% after deductible 20% after deductible
30 Visits
Hospital Services
Inpatient 20% after deductible 20% after deductible
Outpatient 20% after deductible 20% after deductible
Emergency Room 20% after deductible 20% after deductible
* In-network benefits are shown here. For out-of-network coverage details, please
refer to your summary plan description (SPD) or an official plan document.
Please contact benefits@carehere.com to request more information.
5
Plan Details*
BCBST BCBST
Option 1—TN Only Option 2
Network S Network P
Calendar Year Deductible
Individual $2,600 $2,600
Family $5,000 $5,000
Out-of-Pocket Maximum
Individual $4,000 $4,000
Family $8,000 $8,000
Physician Office Visits
Wellness/Preventive Covered at 100% Covered at 100%
Primary Care 20% after deductible 20% after deductible
Specialist 20% after deductible 20% after deductible
Urgent Care 20% after deductible 20% after deductible
Chiropractic Care— 20% after deductible 20% after deductible
30 Visits
Hospital Services
Inpatient 20% after deductible 20% after deductible
Outpatient 20% after deductible 20% after deductible
Emergency Room 20% after deductible 20% after deductible
* In-network benefits are shown here. For out-of-network coverage details, please
refer to your summary plan description (SPD) or an official plan document.
Please contact benefits@carehere.com to request more information.
5