
Page 12 - PHPCN 2019 Annual Conference
P. 12
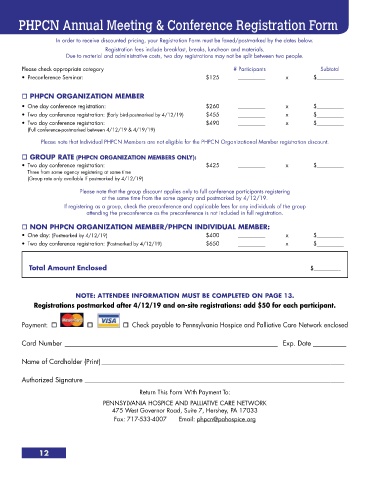
PHPCN Annual Meeting & Conference Registration Form
In order to receive discounted pricing, your Registration Form must be faxed/postmarked by the dates below.
Registration fees include breakfast, breaks, luncheon and materials.
Due to material and administrative costs, two day registrations may not be split between two people.
Please check appropriate category # Participants Subtotal
• Preconference Seminar: $125 __________ x $__________
PHPCN ORGANIZATION MEMBER
• One day conference registration: $260 __________ x $__________
• Two day conference registration: (Early bird-postmarked by 4/12/19) $455 __________ x $__________
• Two day conference registration: $490 __________ x $__________
• (Full conference-postmarked between 4/12/19 & 4/19/19)
Please note that Individual PHPCN Members are not eligible for the PHPCN Organizational Member registration discount.
GROUP RATE (PHPCN ORGANIZATION MEMBERS ONLY):
• Two day conference registration: $425 __________ x $__________
• Three from same agency registering at same time
• (Group rate only available if postmarked by 4/12/19)
Please note that the group discount applies only to full conference participants registering
at the same time from the same agency and postmarked by 4/12/19.
If registering as a group, check the preconference and applicable fees for any individuals of the group
attending the preconference as the preconference is not included in full registration.
NON PHPCN ORGANIZATION MEMBER/PHPCN INDIVIDUAL MEMBER:
• One day: (Postmarked by 4/12/19) $400 __________ x $__________
• Two day conference registration: (Postmarked by 4/12/19) $650 __________ x $__________
Total Amount Enclosed $__________
NOTE: ATTENDEE INFORMATION MUST BE COMPLETED ON PAGE 13.
Registrations postmarked after 4/12/19 and on-site registrations: add $50 for each participant.
Payment: Check payable to Pennsylvania Hospice and Palliative Care Network enclosed
Card Number ________________________________________________________________ Exp. Date __________
Name of Cardholder (Print) _________________________________________________________________________
Authorized Signature ______________________________________________________________________________
Return This Form With Payment To:
PENNSYLVANIA HOSPICE AND PALLIATIVE CARE NETWORK
475 West Governor Road, Suite 7, Hershey, PA 17033
Fax: 717-533-4007 Email: phpcn@pahospice.org
12