
Page 5 - 2022 OCFJSD Benefits Guide
P. 5
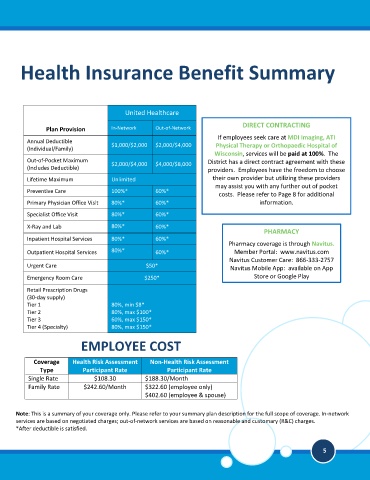
Health Insurance Benefit Summary
United Healthcare
DIRECT CONTRACTING
Plan Provision In-Network Out-of-Network
If employees seek care at MDI Imaging, ATI
Annual Deductible
$1,000/$2,000 $2,000/$4,000 Physical Therapy or Orthopaedic Hospital of
(Individual/Family)
Wisconsin, services will be paid at 100%. The
Out-of-Pocket Maximum $2,000/$4,000 $4,000/$8,000 District has a direct contract agreement with these
(Includes Deductible) providers. Employees have the freedom to choose
Lifetime Maximum Unlimited their own provider but utilizing these providers
may assist you with any further out of pocket
Preventive Care 100%* 60%*
costs. Please refer to Page 8 for additional
Primary Physician Office Visit 80%* 60%* information.
Specialist Office Visit 80%* 60%*
X-Ray and Lab 80%* 60%*
PHARMACY
Inpatient Hospital Services 80%* 60%*
Pharmacy coverage is through Navitus.
Outpatient Hospital Services 80%* 60%* Member Portal: www.navitus.com
Navitus Customer Care: 866-333-2757
Urgent Care $50*
Navitus Mobile App: available on App
Emergency Room Care $250* Store or Google Play
Retail Prescription Drugs
(30-day supply)
Tier 1 80%, min $8*
Tier 2 80%, max $100*
Tier 3 60%, max $150*
Tier 4 (Specialty) 80%, max $150*
EMPLOYEE COST
Coverage Health Risk Assessment Non-Health Risk Assessment
Type Participant Rate Participant Rate
Single Rate $108.30 $188.30/Month
Family Rate $242.60/Month $322.60 (employee only)
$402.60 (employee & spouse)
Note: This is a summary of your coverage only. Please refer to your summary plan description for the full scope of coverage. In-network
services are based on negotiated charges; out-of-network services are based on reasonable and customary (R&C) charges.
*After deductible is satisfied.
5