
Page 7 - Benefit Guide 2022
P. 7
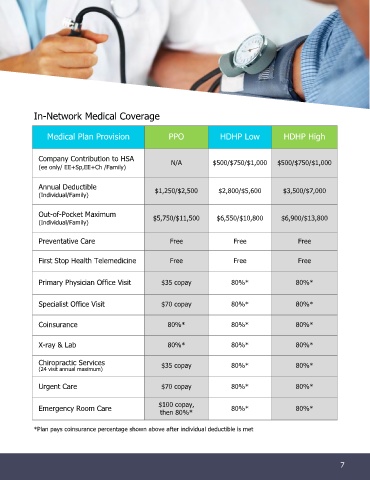
In-Network Medical Coverage
Medical Plan Provision PPO HDHP Low HDHP High
Company Contribution to HSA N/A $500/$750/$1,000 $500/$750/$1,000
(ee only/ EE+Sp,EE+Ch /Family)
Annual Deductible
(Individual/Family) $1,250/$2,500 $2,800/$5,600 $3,500/$7,000
Out-of-Pocket Maximum
(Individual/Family) $5,750/$11,500 $6,550/$10,800 $6,900/$13,800
Preventative Care Free Free Free
First Stop Health Telemedicine Free Free Free
Primary Physician Office Visit $35 copay 80%* 80%*
Specialist Office Visit $70 copay 80%* 80%*
Coinsurance 80%* 80%* 80%*
X-ray & Lab 80%* 80%* 80%*
Chiropractic Services $35 copay 80%* 80%*
(24 visit annual maximum)
Urgent Care $70 copay 80%* 80%*
$100 copay,
Emergency Room Care 80%* 80%*
then 80%*
*Plan pays coinsurance percentage shown above after individual deductible is met
7
7 98