
Page 8 - Benefit Guide 2022
P. 8
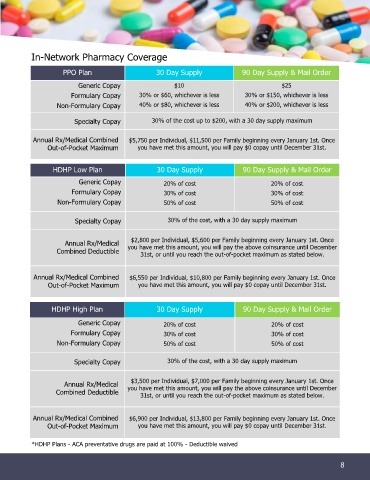
In-Network Pharmacy Coverage
PPO Plan 30 Day Supply 90 Day Supply & Mail Order
Generic Copay $10 $25
Formulary Copay 30% or $60, whichever is less 30% or $150, whichever is less
Non-Formulary Copay 40% or $80, whichever is less 40% or $200, whichever is less
Specialty Copay 30% of the cost up to $200, with a 30 day supply maximum
Annual Rx/Medical Combined $5,750 per Individual, $11,500 per Family beginning every January 1st. Once
Out-of-Pocket Maximum you have met this amount, you will pay $0 copay until December 31st.
HDHP Low Plan 30 Day Supply 90 Day Supply & Mail Order
Generic Copay 20% of cost 20% of cost
Formulary Copay 30% of cost 30% of cost
Non-Formulary Copay 50% of cost 50% of cost
Specialty Copay 30% of the cost, with a 30 day supply maximum
$2,800 per Individual, $5,600 per Family beginning every January 1st. Once
Annual Rx/Medical you have met this amount, you will pay the above coinsurance until December
Combined Deductible 31st, or until you reach the out-of-pocket maximum as stated below.
Annual Rx/Medical Combined $6,550 per Individual, $10,800 per Family beginning every January 1st. Once
Out-of-Pocket Maximum you have met this amount, you will pay $0 copay until December 31st.
HDHP High Plan 30 Day Supply 90 Day Supply & Mail Order
Generic Copay 20% of cost 20% of cost
Formulary Copay 30% of cost 30% of cost
Non-Formulary Copay 50% of cost 50% of cost
Specialty Copay 30% of the cost, with a 30 day supply maximum
$3,500 per Individual, $7,000 per Family beginning every January 1st. Once
Annual Rx/Medical you have met this amount, you will pay the above coinsurance until December
Combined Deductible 31st, or until you reach the out-of-pocket maximum as stated below.
Annual Rx/Medical Combined $6,900 per Individual, $13,800 per Family beginning every January 1st. Once
Out-of-Pocket Maximum you have met this amount, you will pay $0 copay until December 31st.
*HDHP Plans - ACA preventative drugs are paid at 100% - Deductible waived
8
8 98