
Page 60 - Journal of Management Inquiry, July 2018
P. 60
274 Journal of Management Inquiry 27(3)
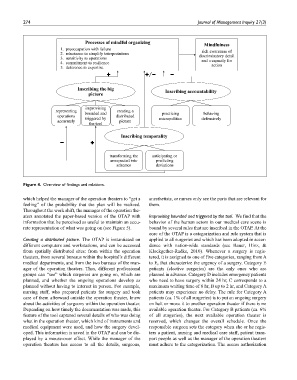
Figure 4. Overview of findings and relations.
which helped the manager of the operation theaters to “get a anesthetists, or nurses only see the parts that are relevant for
feeling” of the probability that the plan will be realized. them.
Throughout the work shift, the manager of the operation the-
aters annotated the paper-based version of the OTAP with Improvising bounded and triggered by the tool. We find that the
information that he perceived as useful to maintain an accu- behavior of the human actors in our medical care scene is
rate representation of what was going on (see Figure 5). bound by several rules that are inscribed in the OTAP. At the
core of the OTAP is a categorization and rule system that is
Creating a distributed picture. The OTAP is instantiated on applied to all surgeries and which has been adopted in accor-
different computers and workstations, and can be accessed dance with nation-wide standards (see Bauer, Hinz, &
from spatially distributed sites: from within the operation Klockgether-Radke, 2010). Whenever a surgery is regis-
theaters, from several bureaus within the hospital’s different tered, it is assigned to one of five categories, ranging from A
medical departments, and from the two bureaus of the man- to E, that characterize the urgency of a surgery. Category E
ager of the operation theaters. Thus, different professional patients (elective surgeries) are the only ones who are
groups can “see” which surgeries are going on, which are planned in advance. Category D includes emergency patients
planned, and whether the ongoing operations develop as who need to have surgery within 24 hr, C corresponds to a
planned without having to interact in person. For example, maximum waiting time of 6 hr, B up to 2 hr, and Category A
nursing staff, who prepared patients for surgery and took patients may experience no delay. The rule for Category A
care of them afterward outside the operation theater, knew patients (ca. 1% of all surgeries) is to put an ongoing surgery
about the activities of surgeons within the operation theater. on halt or move it to another operation theater if there is no
Depending on how timely the documentation was made, this available operation theater. For Category B patients (ca. 6%
feature of the tool captured several details of who was doing of all surgeries), the next available operation theater is
what in the operation theater, which kind of instruments and reserved, which changes the overall schedule. Once the
medical equipment were used, and how the surgery devel- responsible surgeon sets the category when she or he regis-
oped. This information is saved in the OTAP and can be dis- ters a patient, nursing and medical care staff, patient trans-
played by a mouse-over effect. While the manager of the port people as well as the manager of the operation theaters
operation theaters has access to all the details, surgeons, must adhere to the categorization. The access authorization