
Page 18 - Allegacy 2017 booklet 8.5x11
P. 18
Allegacy Benefit Solutions Page 18
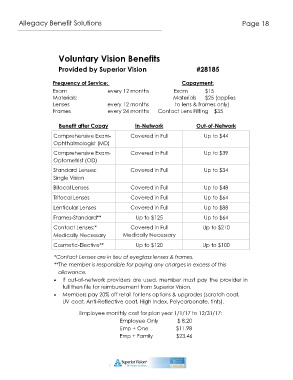
Voluntary Vision Benefits
Provided by Superior Vision #28185
Frequency of Service: Copayment:
Exam every 12 months Exam $15
Materials: Materials $25 (applies
Lenses every 12 months to lens & frames only)
Frames every 24 months Contact Lens Fitting $35
Benefit after Copay In-Network Out-of-Network
Comprehensive Exam- Covered in Full Up to $44
Ophthalmologist (MD)
Comprehensive Exam- Covered in Full Up to $39
Optometrist (OD)
Standard Lenses: Covered in Full Up to $34
Single Vision
Bifocal Lenses Covered in Full Up to $48
Trifocal Lenses Covered in Full Up to $64
Lenticular Lenses Covered in Full Up to $88
Frames-Standard** Up to $125 Up to $64
Contact Lenses:* Covered in Full Up to $210
Medically Necessary Medically Necessary
Cosmetic-Elective** Up to $120 Up to $100
*Contact Lenses are in lieu of eyeglass lenses & frames.
**The member is responsible for paying any charges in excess of this
allowance.
If out-of-network providers are used, member must pay the provider in
full then file for reimbursement from Superior Vision.
Members pay 20% off retail for lens options & upgrades (scratch coat,
UV coat, Anti-Reflective coat, High Index, Polycarbonate, tints).
Employee monthly cost for plan year 1/1/17 to 12/31/17:
Employee Only $ 8.20
Emp + One $11.98
Emp + Family $23.46