
Page 116 - Medicine and Surgery
P. 116
P1: FAW
BLUK007-03 BLUK007-Kendall May 25, 2005 17:29 Char Count= 0
112 Chapter 3: Respiratory system
Management of acute severe asthma in adults in A&E
Measure Peak Expiratory Flow and Arterial Saturations
Time
PEF >75% best or predicted PEF 33–75% best or predicted PEF <33% best or predicted
mild moderate – severe: OR any life threatening features:
features of severe asthma • SpO2 <92%
• PEF <50% best or predicted
• Respiration ≥25/min • Silent chest, cyanosis, poor respiratory effort
• Pulse ≥110 breaths/min • Bradycardia, arrhythmia, hypotension
• Cannot complete sentence in one breath • Exhaustion, confusion, coma
Obtain senior/ICU help now if any
5 mins Give usual bronchodilator Give salbutamol 5 mg by oxygen-driven nebuliser
life-threatening features are present
IMMEDIATE MANAGEMENT
• High concentration oxygen (>60% if possible)
• Give salbutamol 5 mg plus ipratropium 0.5 mg via
No life threatening Life threatening oxygen-driven nebuliser
15–30 Clinically stable Clinically stable
mins AND PEF >75% AND PEF <75% features features • AND prednisolone 40–50 mg orally or IV
AND PEF 50–75% OR PEF <50% hydrocortisone 100 mg
Repeat salbutamol 5 mg nebuliser Measure arterial blood gases
Give prednisolone Markers of severity:
40–50 mg orally - Normal or raised PaCO 2
(Pa CO 2 >4.6 kPa; 35 mmHg)
- Severe hypoxia
(PaO 2 <8 kPa; 60 mmHg)
- Low pH (or high H + )
No signs of severe Signs of severe
Patient recovering • Give/repeat salbutamol 5 mg with ipratropium 0.5 mg
60 mins asthma asthma
AND PEF >75% by oxygen-driven nebuliser after 15 minutes
AND PEF 50–75% OR PEF <50%
• Consider continuous salbutamol nebuliser 5–10 mg/hr
• Consider IV magnesium sulphate 1.2–2 g over 20
OBSERVE
monitor SpO 2 , heart rate and respiratory rate minutes
• Correct fluid/electrolytes, especially K + disturbances
• Chest x-ray
Signs of severe ADMIT
Patient stable
120 mins asthma Patient should be accompanied by a
AND PEF >50%
OR PEF <50% nurse or doctor at all times
Peak expiratory flow in normal adults
660 660
650 75 190 650
640 72 183 640
630 69 175 MEN 630
620 66 167 620
610 63 160 610
Ht. Ht.
600 (ins) (cms) 600
590 590
580 580
570 570
560 560
550 550
540 STANDARD DEVIATION MEN 48 = litres/min 540
530 STANDARD DEVIATION WOMEN 42 = litres/min 530
PEF 520 520
L/min 510 510
500 500
490 69 175 WOMEN 490
66 167
480 480
POTENTIAL DISCHARGE 470 63 160 470
460 60 152 460
• In all patients who received nebulised β 2 agonists prior to 450 57 Ht. 145 Ht. 450
presentation, consider an extended observation period prior 440 (ins) (cms) 440
430
430
to discharge 420 IN MEN VALUES OF PEF UP TO 100 LITRES/MIN LESS THAN 420
• If PEF < 50% on presentation, prescribe prednisolone 40–50 410 PREDICTED, AND IN WOMEN LESS THAN 85 LITRES/MIN LESS 410
mg/day for 5 days 400 THAN PREDICTED, ARE WITHIN NORMAL LIMITS. 400
• In all patients ensure treatment supply of inhaled steroid and 390 390
380 380
β 2 agonist and check inhaler technique
• Arrange GP follow up for 2 days post presentation
• Fax discharge letter to GP 15 20 25 30 35 40 45 50 55 60 65 70
• Refer to asthma liaison nurse/chest clinic AGE IN YEARS
Nunn AJ, Gregg I. New regression equations for predicting
peak expiratory flow in adults. BMJ 1989;298;1068–70.
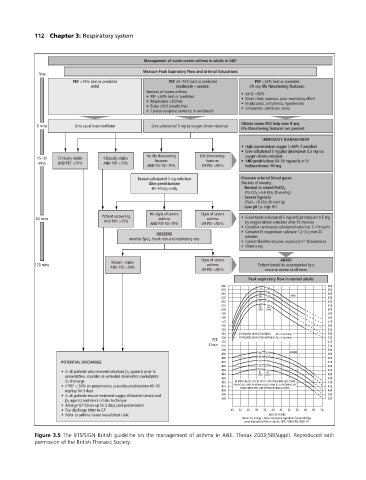
Figure 3.5 The BTS/SIGN British guideline on the management of asthma in A&E. Thorax 2003;58(Suppl). Reproduced with
permission of the British Thoracic Society.