
Page 4 - Northbridge Companies 2018 OE Guide_Fomatting corrections (002)HLD
P. 4
If you want medical coverage you must enroll via the Paycom
self service. PCP info required on HMO plan.
Medical Plan Options
ELECTIONS & FORMS ARE DUE DEC. 8, 2017
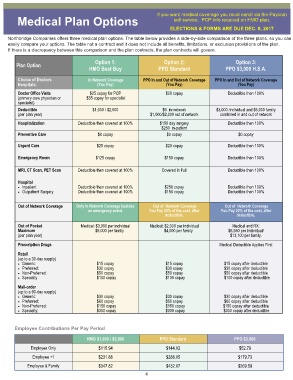
Northbridge Companies offers three medical plan options. The table below provides a side-by-side comparison of the three plans, so you can
easily compare your options. The table not a contract and it does not include all benefits, limitations, or exclusion provisions of the plan.
If there is a discrepancy between this comparison and the plan contracts, the plan contracts will govern.
Option 1: Option 2: Option 3:
Plan Option
HMO Best Buy PPO Standard PPO $3,000 H.S.A.
Choice of Doctors In Network Coverage PPO In and Out of Network Coverage PPO In and Out of Network Coverage
Hospitals: (You Pay) (You Pay) (You Pay)
Doctor Office Visits $25 copay for PCP $20 copay Deductible then 100%
(primary care physician or $35 copay for specialist
specialist)
Deductible $1,000 / $2,000 $0 in-network $3,000 /individual and $6,000 family
(per plan year) $1,000/$2,000 out of network combined in and out of network
Hospitalization Deductible then covered at 100% $150 day surgery Deductible then 100%
$250 in-patient
Preventive Care $0 copay $0 copay $0 copay
Urgent Care $25 copay $20 copay Deductible then 100%
Emergency Room $125 copay $150 copay Deductible then 100%
MRI, CT Scan, PET Scan Deductible then covered at 100% Covered in Full Deductible then 100%
Hospital
• Inpatient Deductible then covered at 100% $250 copay Deductible then 100%
• Outpatient Surgery Deductible then covered at 100% $150 copay Deductible then 100%
Out of Network Coverage Only In Network Coverage besides Out of Network Coverage Out of Network Coverage
an emergency event. You Pay 20% of the cost, after You Pay 20% of the cost, after
deductible. deductible.
Out of Pocket Medical: $3,000 per individual Medical: $2,000 per individual Medical and RX:
Maximum $6,000 per family $4,000 per family $6,550 per individual/
(per plan year) $13,100 per family.
Prescription Drugs Medical Deductible Applies First
Retail
(up to a 30-day supply)
• Generic: $15 copay $15 copay $15 copay after deductible
• Preferred: $30 copay $30 copay $30 copay after deductible
• Non-Preferred: $50 copay $50 copay $50 copay after deductible
• Specialty $100 copay $100 copay $100 copay after deductible
Mail-order
(up to a 90-day supply)
• Generic: $30 copay $30 copay $30 copay after deductible
• Preferred: $60 copay $60 copay $60 copay after deductible
• Non-Preferred: $150 copay $150 copay $150 copay after deductible
• Specialty: $300 copay $300 copay $300 copay after deductible
Employee Contributions Per Pay Period
HMO $1,000 / $2,000 PPO Standard PPO $3,000
Employee Only $115.94 $144.02 $52.79
Employee +1 $231.88 $288.05 $179.73
Employee & Family $347.82 $432.07 $269.59
4