
Page 9 - Northbridge Companies 2018 OE Guide_Fomatting corrections (002)HLD
P. 9
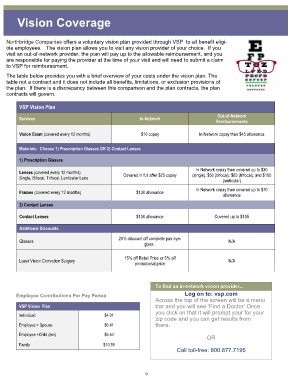
Vision Coverage
Northbridge Companies offers a voluntary vision plan provided through VSP to all benefit eligi-
ble employees. The vision plan allows you to visit any vision provider of your choice. If you
visit an out-of-network provider, the plan will pay up to the allowable reimbursement, and you
are responsible for paying the provider at the time of your visit and will need to submit a claim
to VSP for reimbursement.
The table below provides you with a brief overview of your costs under the vision plan. The
table not a contract and it does not include all benefits, limitations, or exclusion provisions of
the plan. If there is a discrepancy between this comparison and the plan contracts, the plan
contracts will govern.
VSP Vision Plan
Out-of-Network
Services In-Network
Reimbursements
Vision Exam (covered every 12 months) $10 copay In Network copay then $45 allowance
Materials: Choose 1) Prescription Glasses OR 2) Contact Lenses
1) Prescription Glasses
In Network copay then covered up to $30
Lenses (covered every 12 months)
Single, Bifocal, Trifocal, Lenticular Lens Covered in full after $25 copay (single), $50 (bifocal). $65 (trifocal), and $100
(lenticular)
In Network copay then covered up to $70
Frames (covered every 12 months) $130 allowance
allowance
2) Contact Lenses
Contact Lenses $130 allowance Covered up to $105
Additional Discounts
20% discount off complete pair eye-
Glasses N/A
glass .
15% off Retail Price or 5% off
Laser Vision Correction Surgery N/A
promotional price
To find an in-network vision provider...
Employee Contributions Per Pay Period Log on to: vsp.com
Across the top of the screen will be a menu
VSP Vision Plan bar and you will see ‘Find a Doctor’ Once
you click on that it will prompt your for your
Individual: $4.01
zip code and you can get results from
Employee + Spouse $6.41 there.
Employee +Child (ren) $6.54
OR
Family $10.56
Call toll-free: 800.877.7195
9